
Abdominal and Pelvic Radiology — MCQs

On this page
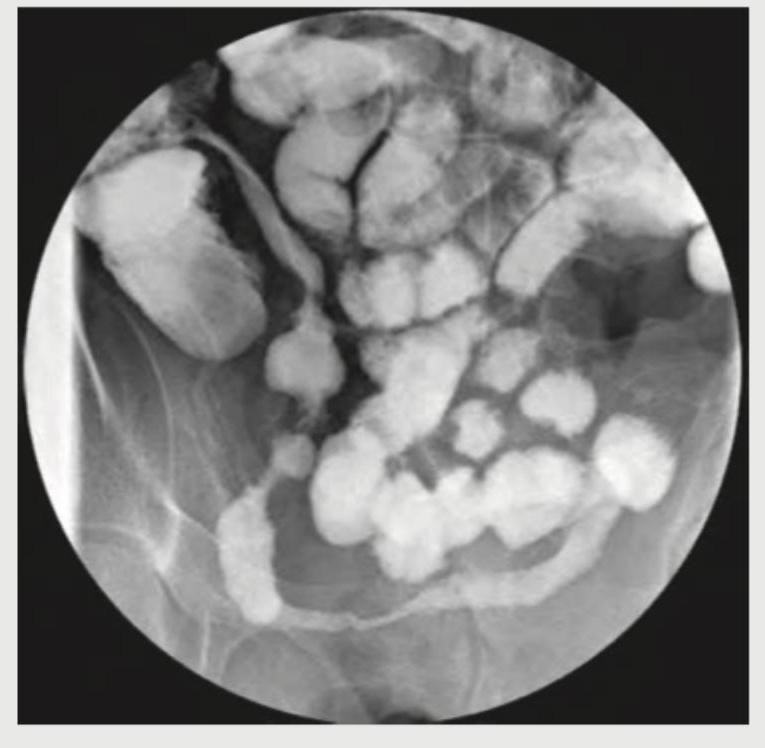
What is the radiological sign demonstrated in the image provided?
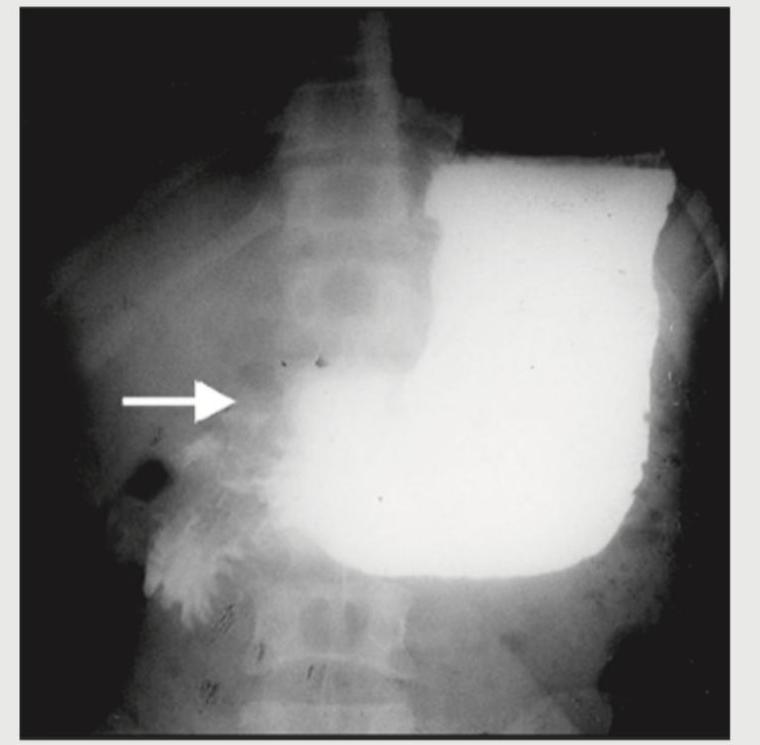
What is the diagnosis based on the barium meal study shown below?
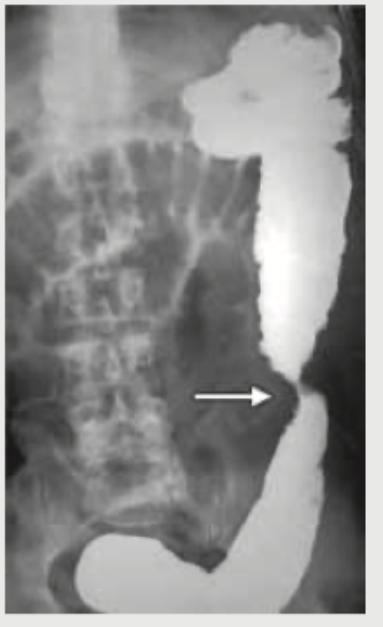
A 62-year-old male presented with signs and symptoms of intestinal obstruction. Radiological image of the patient is given. What is the sign that is illustrated in the image?
A 26-year-old construction worker with a history of long-term analgesic abuse presents with flank pain. What is the radiological sign demonstrated in the IVP image shown below?

What is the radiological sign shown in the image?

What is the radiological sign that could best describe this image?

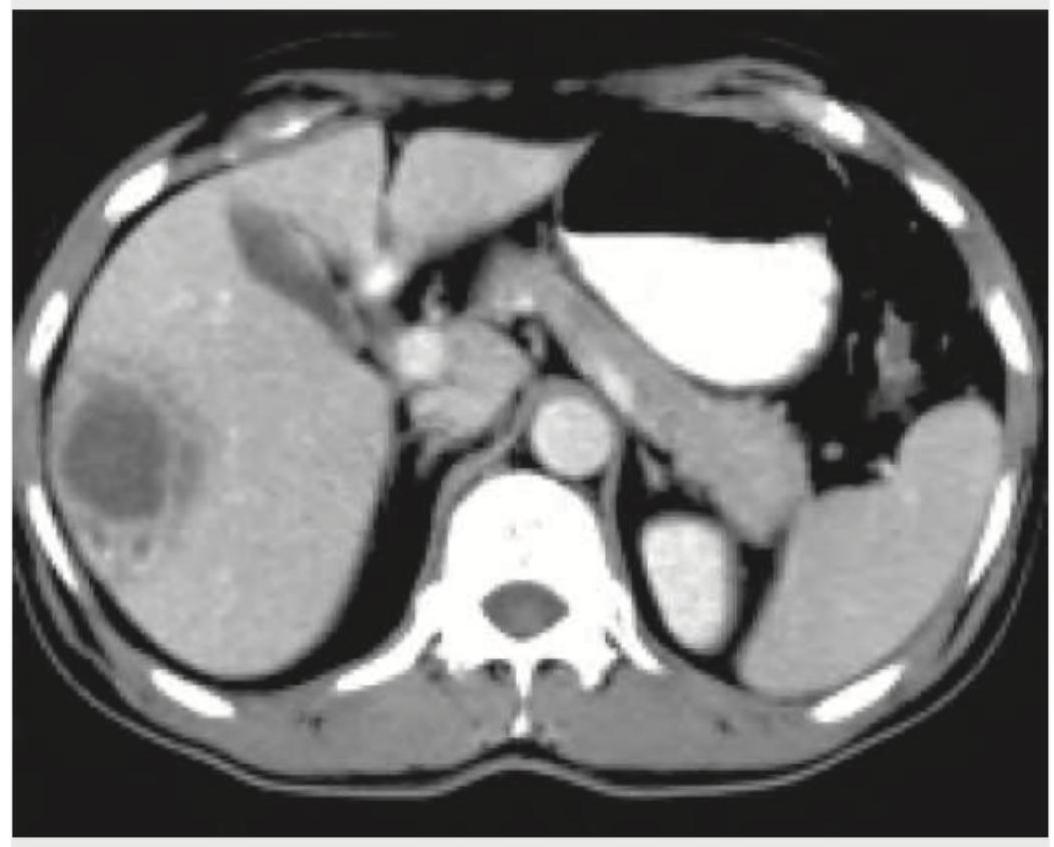
The given CT abdomen shows:

CECT abdomen of a patient with acute abdomen is given below. What is the diagnosis?
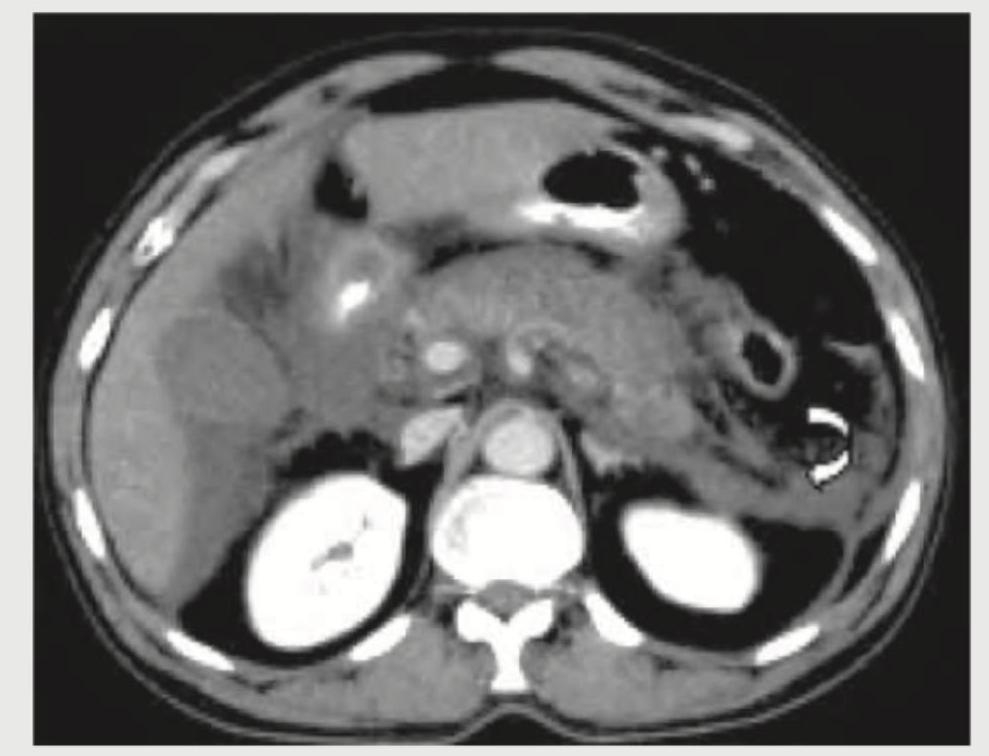
The CT abdomen of a 10-year-old child with high grade fever for last 5 days shows:
A 25-year-old patient underwent surgery for scoliosis correction. 5 days post-operatively he develops voluminous bilious vomiting. The given CT abdomen shows:

Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app