
Abdominal and Pelvic Radiology — MCQs

On this page
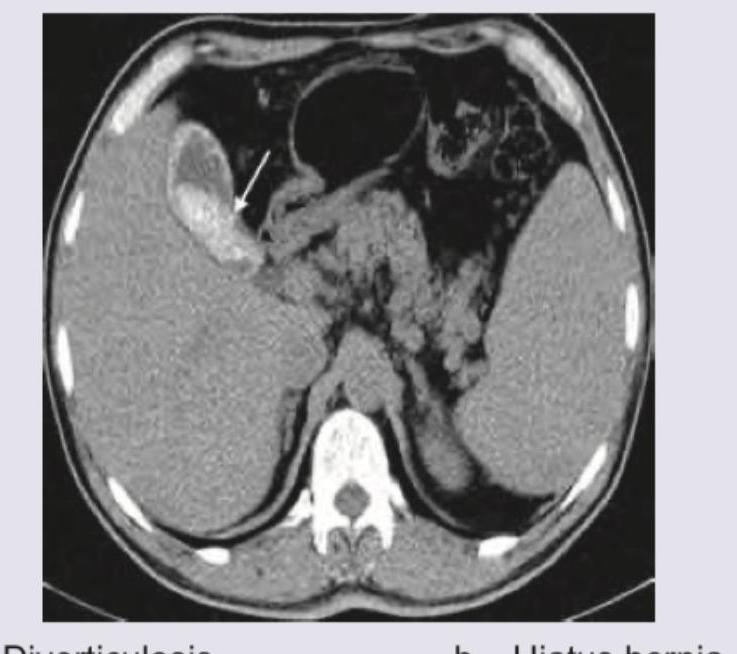
The image shows:

CT abdomen shows: (Recent NEET Pattern 2016-17)
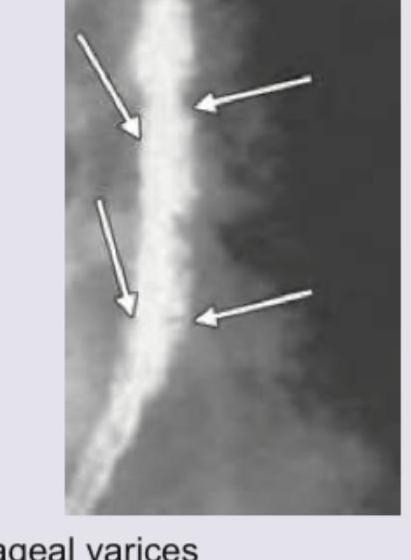
The barium swallow shows presence of:

The following image shows:
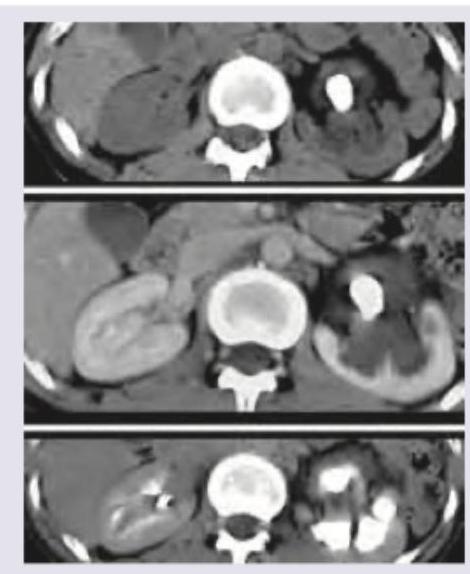
The following urinary bladder on MCU is diagnostic of:

The following barium swallow study shows which of the following?
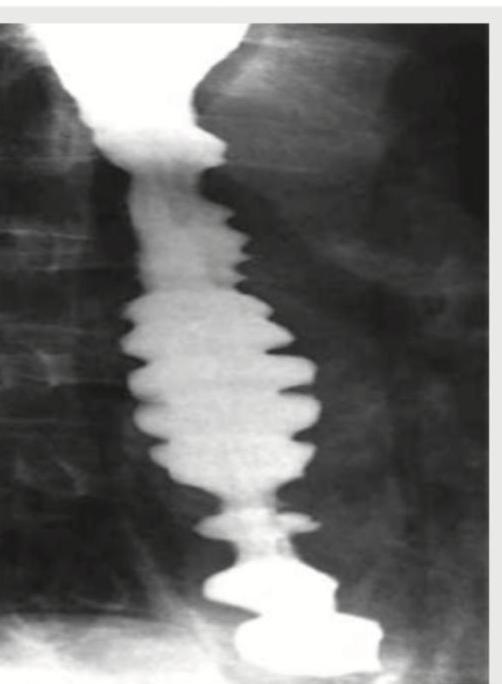
A 45-year-old female patient complains of dysphagia for one year. UGI endoscopy was normal. Diagnosis is: (Recent NEET Pattern 2016-17)

A patient complains of episodes of dysphagia and chest pain. The barium study presentation of the patient is shown below. A radiologist will describe this condition as all except:
A patient presents with abdominal pain, diarrhea and weight loss. He gives a history of taking treatment for pulmonary TB. What does the barium film of the patient show?

Which of the following is shown in the barium study?

Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app