
Abdominal and Pelvic Radiology — MCQs

On this page
A patient presents with abdominal pain, diarrhea and weight loss. He gives past history of pulmonary TB. Barium film of the patient indicates which of the following condition?

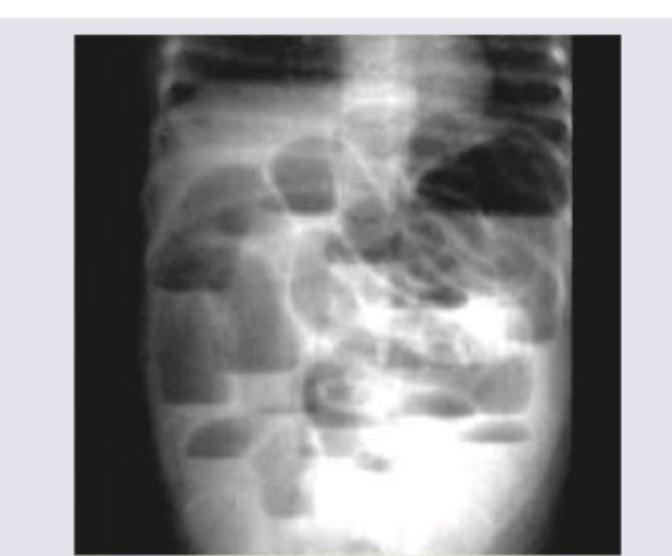
A 28-year-old male patient presents with colicky abdominal pain along with vomiting. X-ray abdomen shows:
This young patient presented with acute right lower abdominal pain. What is the possible diagnosis?

The given barium enema is diagnostic of:

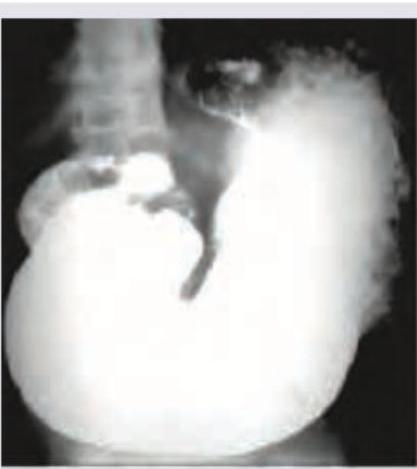
The following barium meal shows:
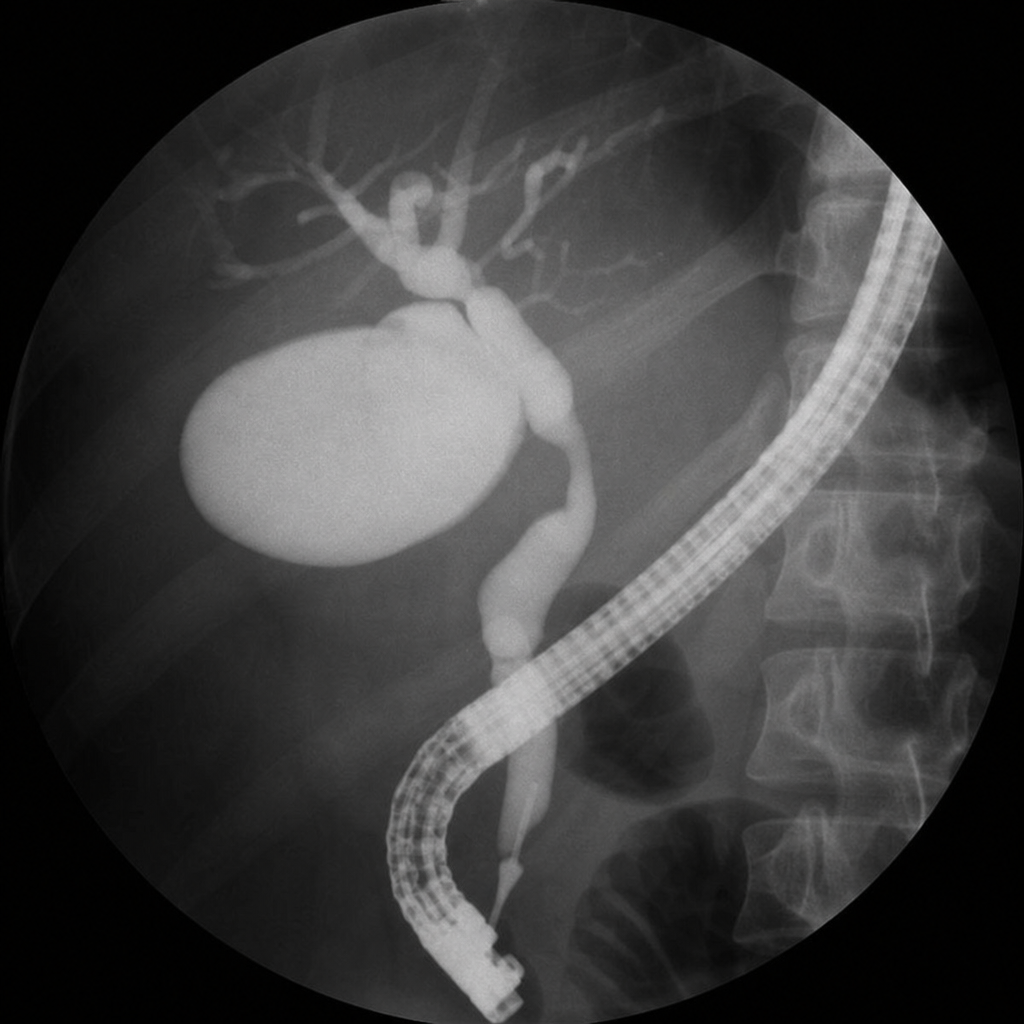
The following ERCP report is diagnostic of:
A 50-year-old man went for his annual medical check-up. CT scan is shown below. Diagnosis is?

The following image shows the presence of?

Identify the grade of vesico-ureteric reflux in the picture below?

An abdominal X-ray of a patient with ulcerative colitis shows peripheral placed bowel dilatations with loss of haustrations. The transverse colon diameter measures 7 cm. The patient has a fever of 38.9°C, heart rate of 112 bpm, and leukocytosis. The image shown is characteristic of:
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app