
Abdominal and Pelvic Radiology — MCQs

On this page
Reflex nephropathy is diagnosed mainly by:
Imaging studies of a patient with a genetic disorder shows the 'central dot sign'. Which condition is characteristic of this finding?
Which of the following imaging findings is diagnostic of Adenomyosis?
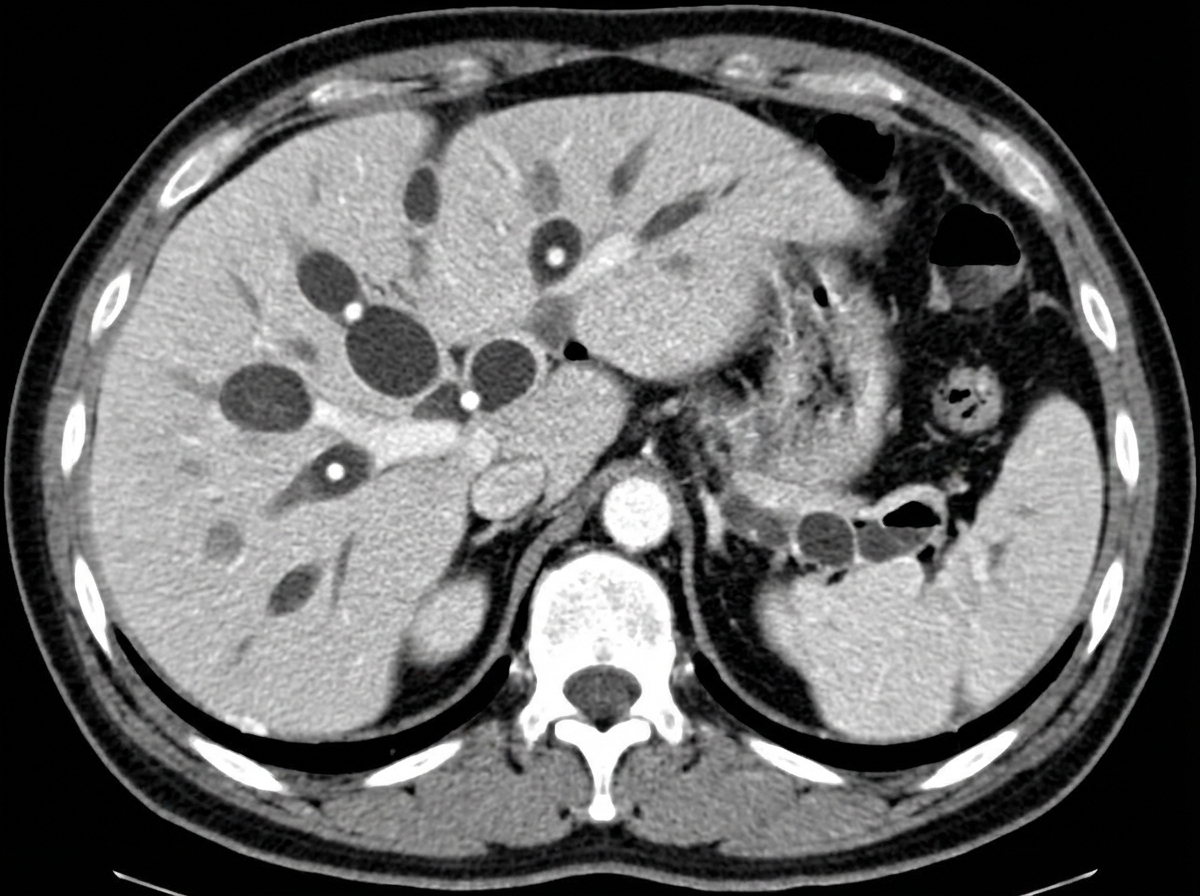
A 10-year-old female presented with recurrent attacks of cholangitis. CECT was done; what is the most likely diagnosis based on CECT findings?
A liver lesion showing multiseptate cystic areas with eggshell or mural calcifications on CT scan is suggestive of?
A patient presents with recent loss of hypertension control and a creatinine of 4.2 mg/dL. Renal ultrasound shows size discrepancy in the kidneys and no signs of obstruction. What should be the next investigation?
A lobulated mass extending into the gastric bubble with rat tail tapering of the lower esophagus in a barium swallow is indicative of which condition?
Micturating cystourethrogram is not used in which of the following conditions?
Fir tree appearance of the bladder is seen in which condition?
Which of the following imaging techniques is NOT used for the evaluation of uterine anomalies?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app