
Abdominal and Pelvic Radiology — MCQs

On this page
A 55-year-old male patient presents with hematuria and a mass in the left kidney on a CT scan, as shown below. What is the diagnosis?
Identify the investigation modality shown in the image.
The Sonographic scan given below shows:

Which of the following kidney stones best explains the findings in this X-ray KUB?

Identify the radiological investigation and finding shown in the image below:

The following contrast-enhanced CT image shows:

The following IVU shows:

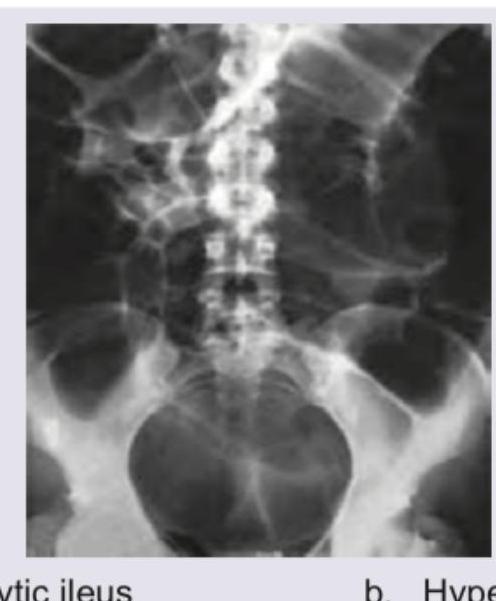
The radiographic findings are most consistent with:
All of the following can be used to describe the radiological image shown below EXCEPT:

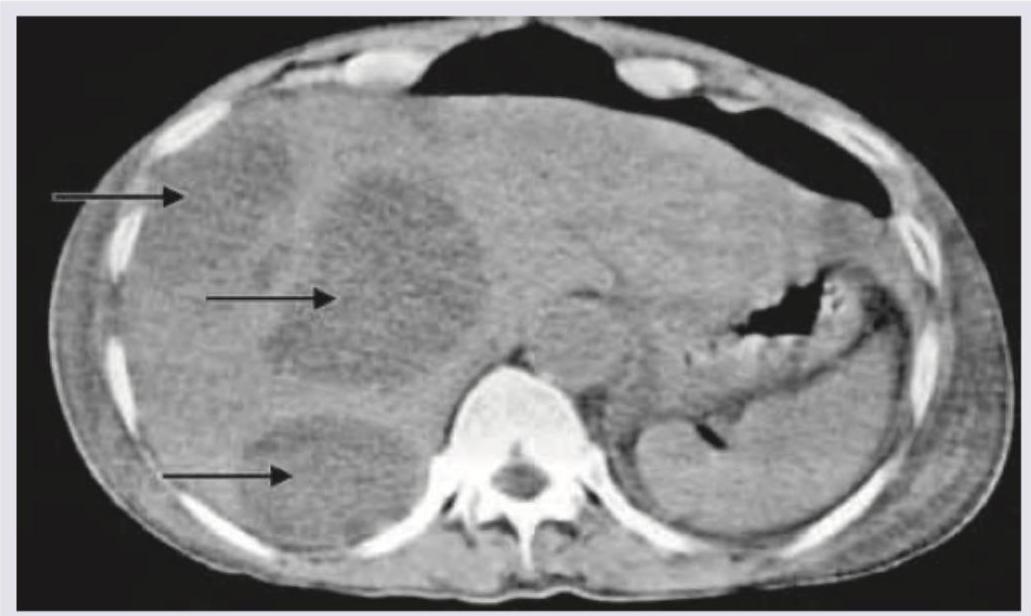
What does the given CT abdomen show?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app