
Abdominal and Pelvic Radiology — MCQs

On this page
An asymptomatic male presented for ultrasonography of the abdomen for medical fitness. A focal lesion was found in his liver on ultrasound. The patient was informed that this is the most common benign hepatic tumor. Which of the following is a false statement about this lesion?
A 24-year-old man presented with a retroperitoneal, necrotic, heterogeneously enhancing mass on CT near the hilum of the left kidney. What is the most probable diagnosis?
A hysterosalpingogram was performed for infertility evaluation and revealed the appearance shown here. What is the diagnosis?

Which of the following is NOT a true feature of ileocecal tuberculosis on a diagnostic barium follow-through examination?
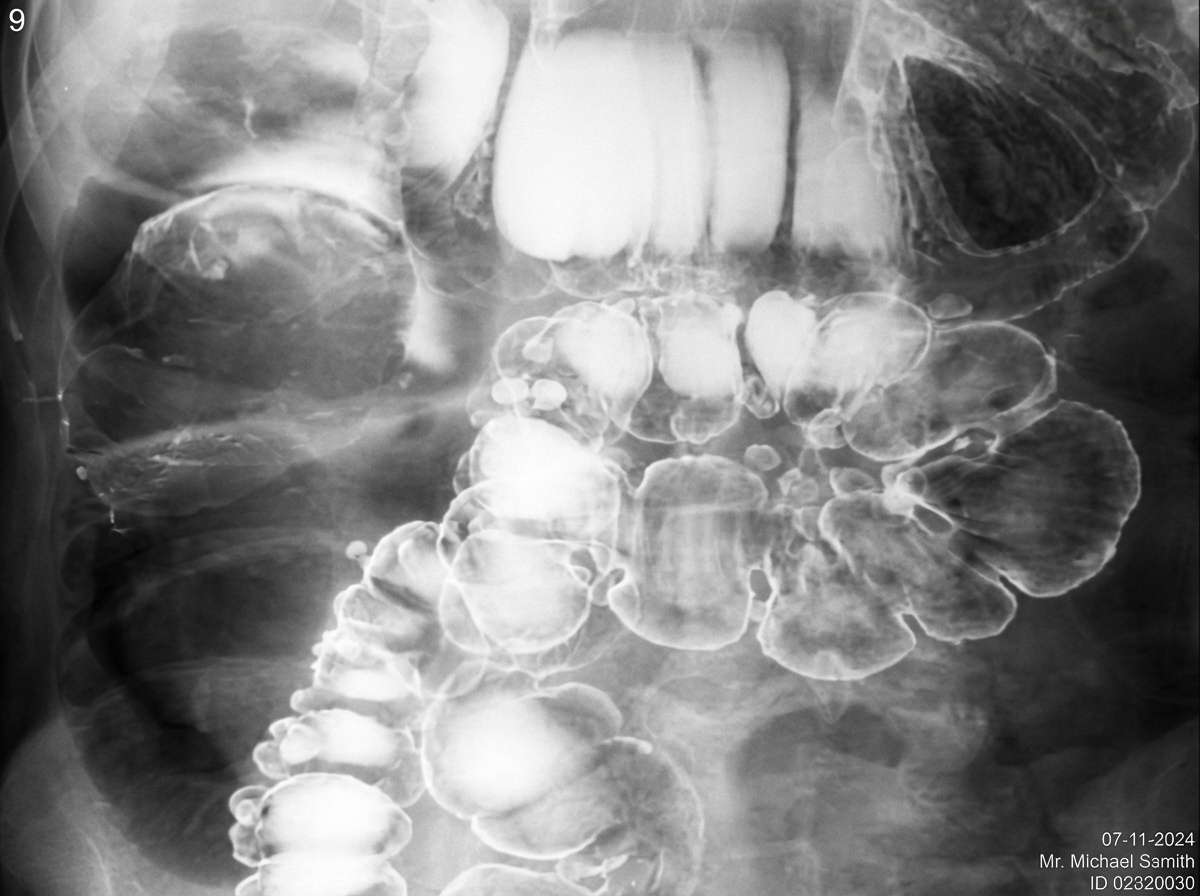
What condition is suggested by the following appearance on a barium enema?
Gooseneck deformity is seen in which of the following conditions?
Which one of the following organs is enlarged?

What is the investigation of choice to visualize gallbladder pathologies?
Which of the following is the best view for visualizing minimal pneumoperitoneum?
On barium swallow, what characteristic appearance is shown by a leiomyoma?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app