
Abdominal and Pelvic Radiology — MCQs

On this page
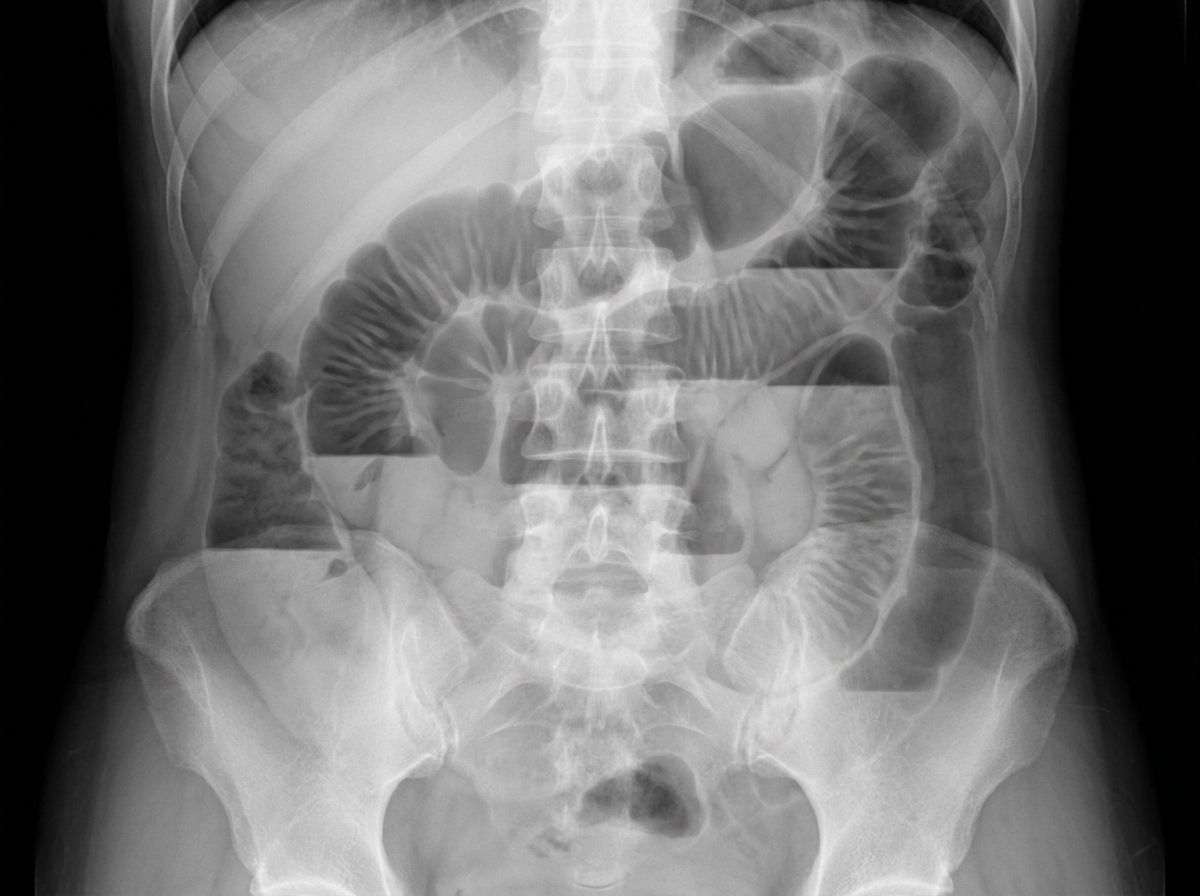
A 30-year-old patient presents with acute abdominal pain and obstipation. An X-ray is provided. What is the most likely diagnosis?
Gas in the biliary tree on plain abdominal X-ray is suggestive of which of the following conditions?
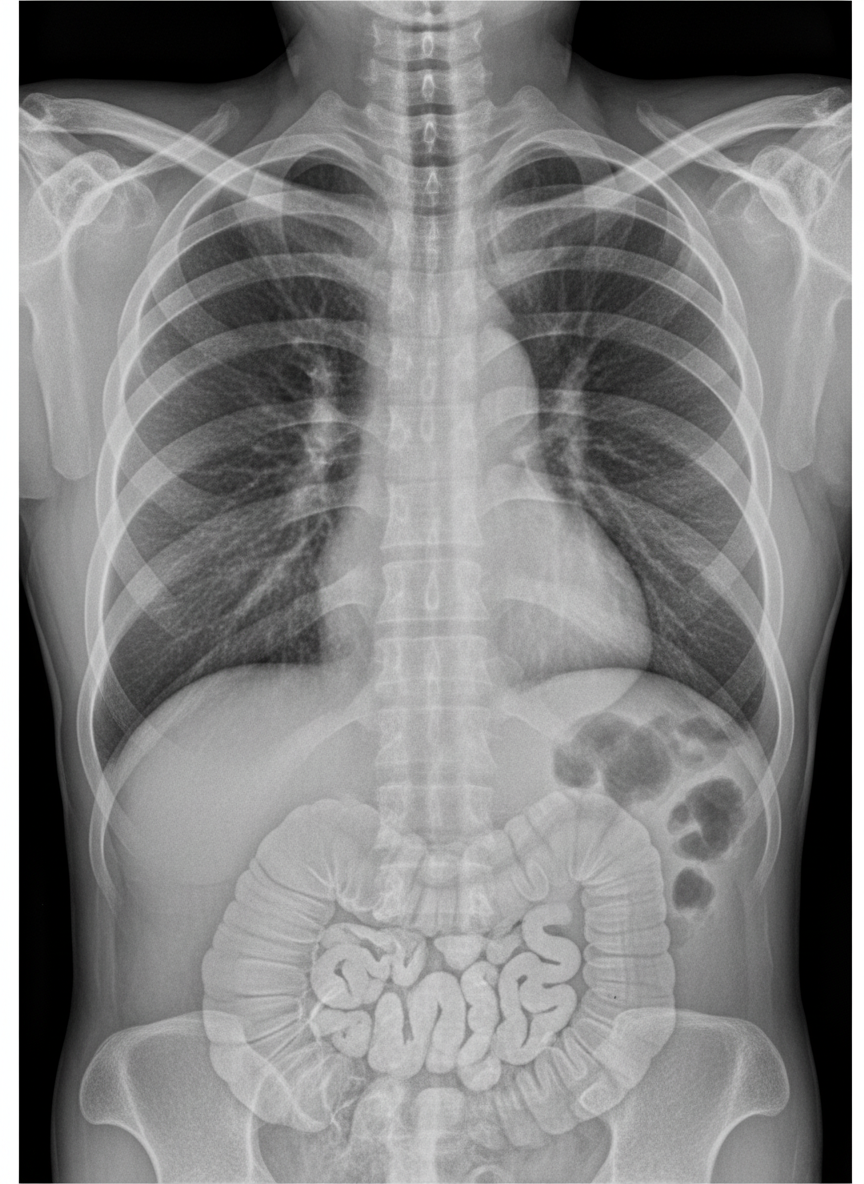
A 24-year-old man presents to the emergency department with a 12-hour history of intermittent, crampy abdominal pain and five episodes of vomiting. He denies any rectal bleeding. On examination, his abdomen is distended with absent bowel sounds. Per-rectal examination is normal. An abdominal X-ray reveals findings suggestive of a specific condition. Based on the X-ray findings, which of the following statements are true? (Select all that apply)

Semen analysis of a young man presenting with primary infertility revealed low volume, fructose-negative ejaculate with azoospermia. Which of the following is the most useful imaging modality to evaluate the cause of his infertility?
Which of the following is a specific diagnostic criterion for Budd-Chiari syndrome?
Which imaging modality is BEST used to detect distant metastasis in pancreatic cancer?
What is the diagnosis suggested by the intravenous urogram (IVU) study?

Early arterial phase enhancement on CECT scan of the liver indicates which of the following?
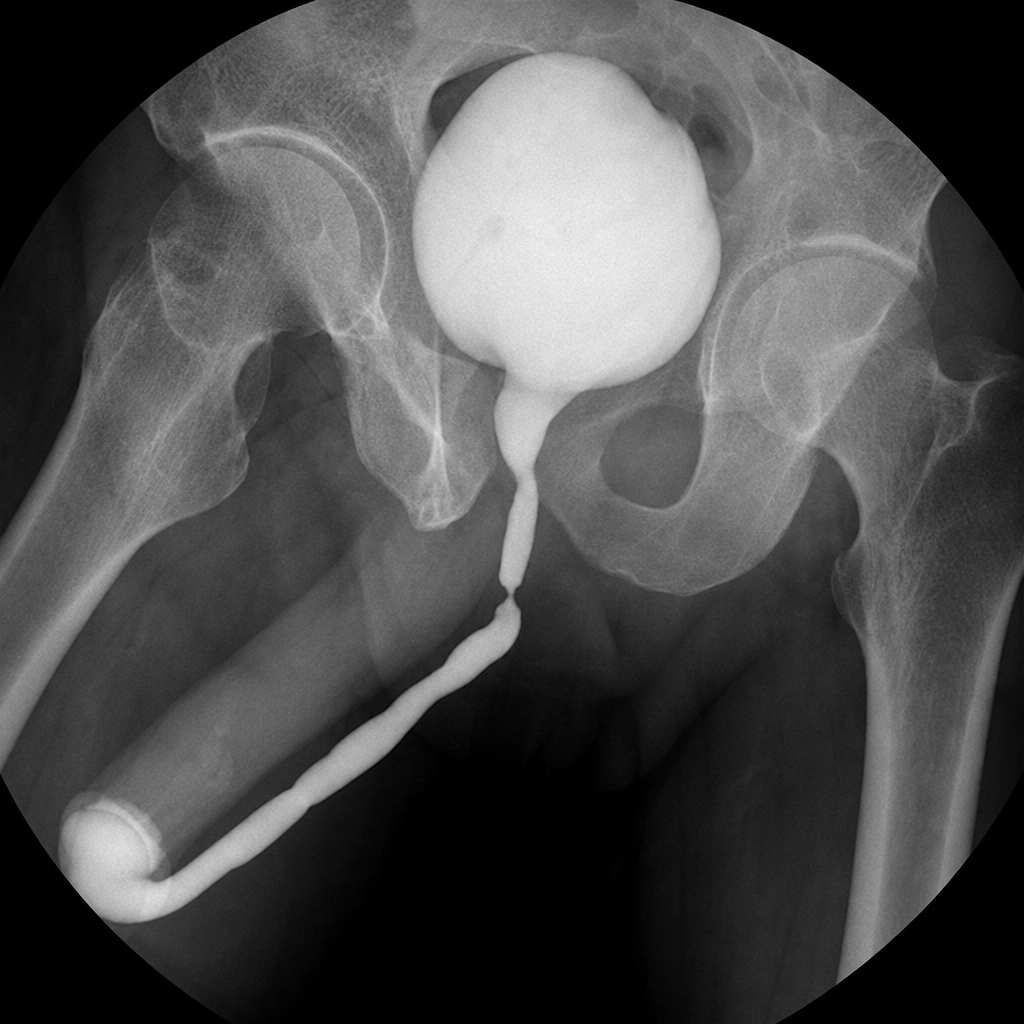
What is the location of the stricture in the given RGU?
An X-ray shows findings suggestive of:
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app