
Abdominal and Pelvic Radiology — MCQs

On this page
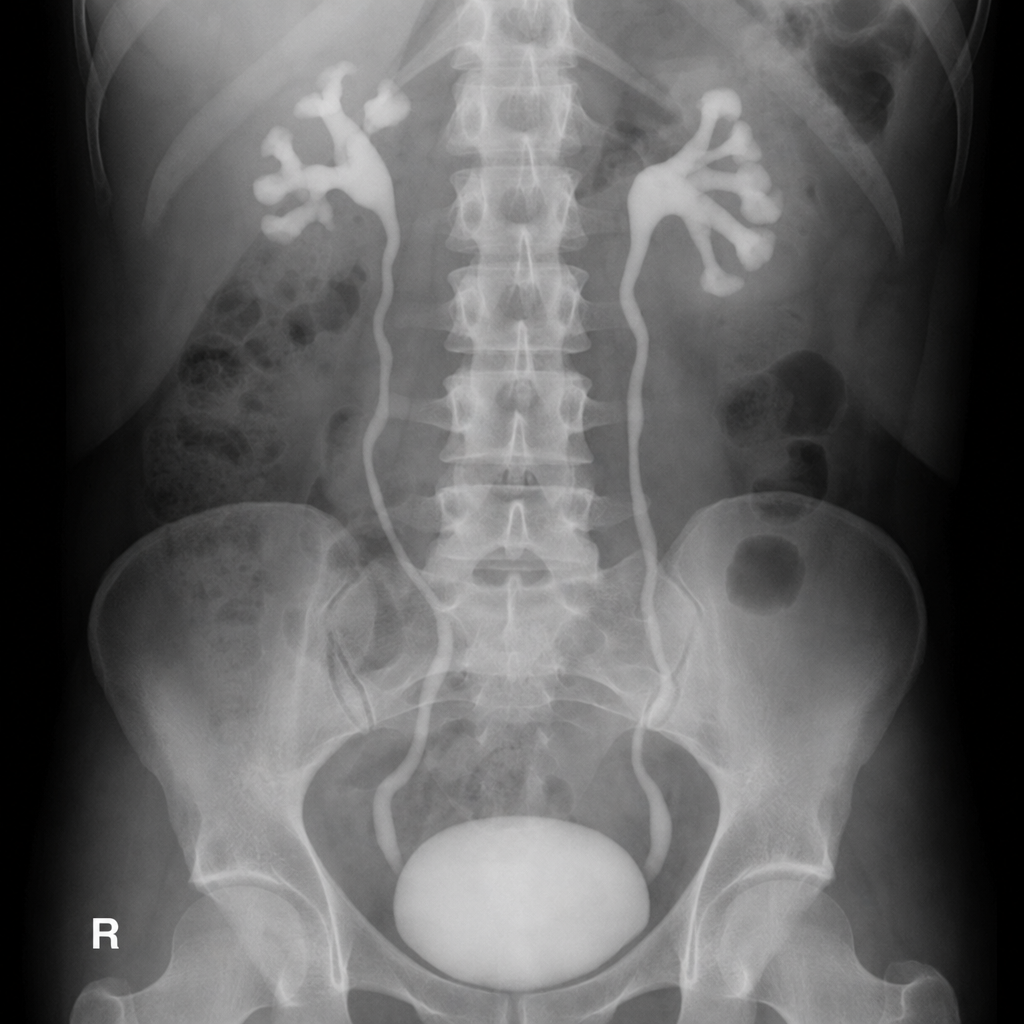
Comment on the diagnosis shown below?
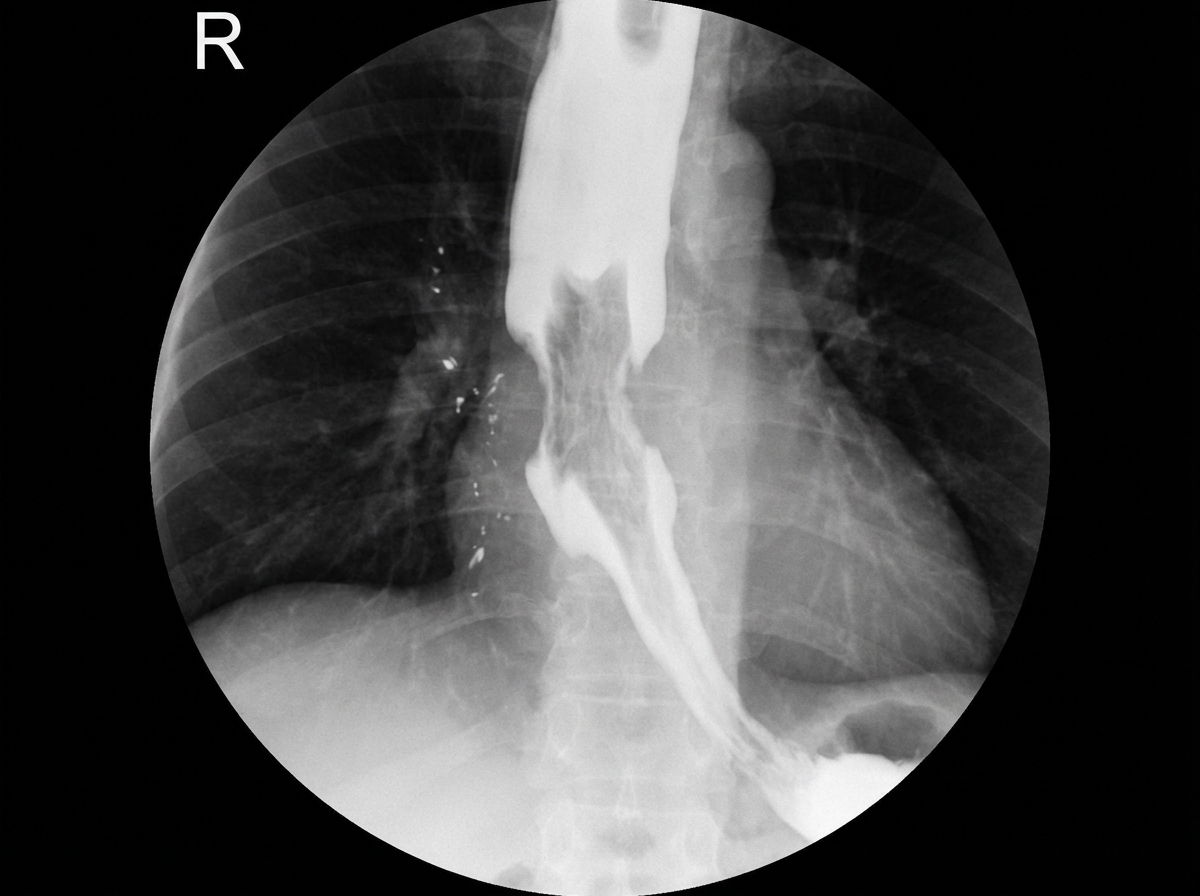
What is the diagnosis suggested by the barium X-ray findings?
What is the first radiologic sign of Crohn's disease in the terminal ileum?
A 61-year-old man undergoes a CT scan study of the abdomen for unexplained abdominal distension. Low attenuation intraperitoneal collections with enhancing septae are demonstrated. There is scalloping of the liver border and omental thickening. Which one of the following is most likely to be the underlying cause?
What is this appearance, seen in early pregnancy, known as?

What is the initial investigation for suspected gallbladder stones?
Which investigation is most sensitive for detecting minimal intraperitoneal free air?
Which pattern is seen in the jejunum on an X-ray?
A 30-year-old female presents with right hypochondrial pain. CT scan reveals floating membranes in the liver. What is the most likely diagnosis?
Radiographic findings of cardiac achalasia include all except?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app