
Abdominal and Pelvic Radiology — MCQs

On this page
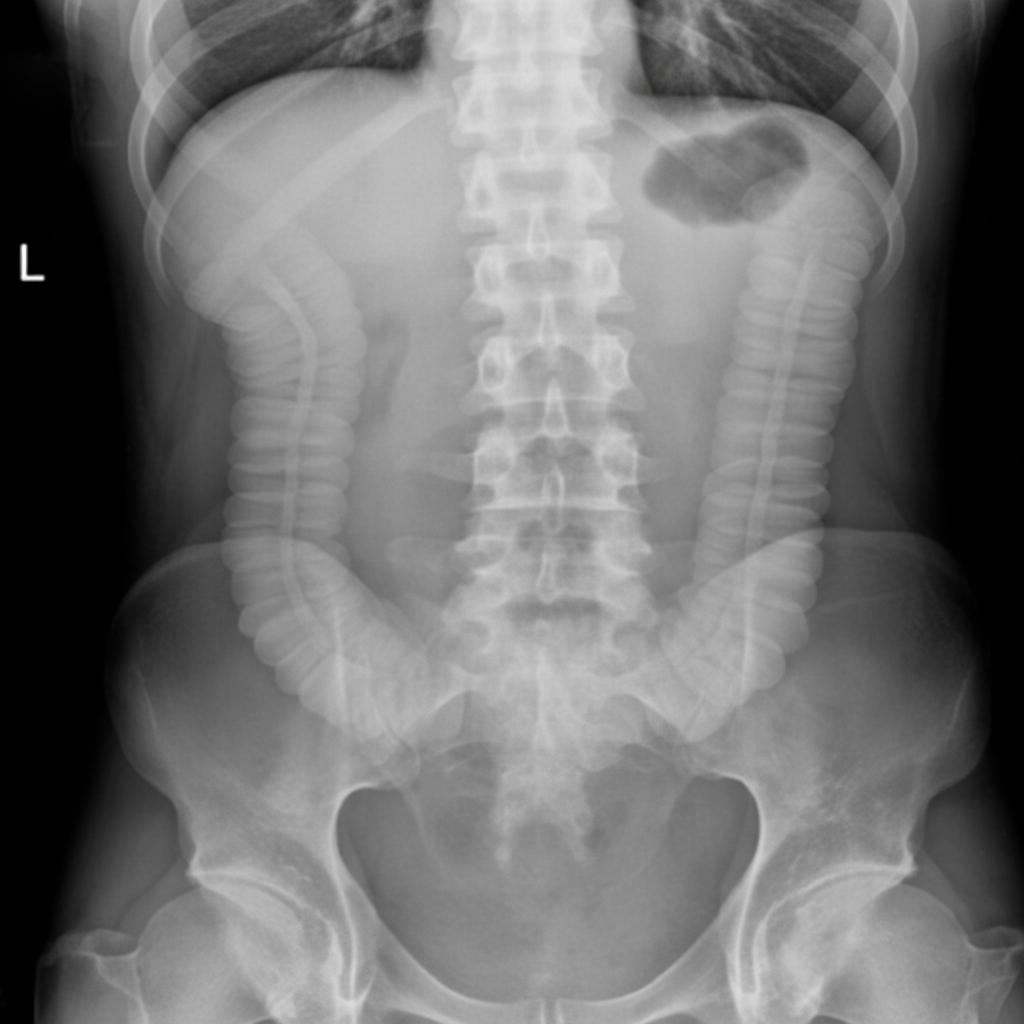
The given image shows findings most consistent with which of the following conditions?
What is the investigation of choice for renovascular hypertension?
The String sign is seen in which of the following conditions?
For purely diagnostic purposes, what is the preferred mode of visualizing the biliary tree?
What is the investigation of choice for acute cholecystitis?
Light bulb appearance in MRI scan is/are seen in which of the following conditions?
The "Rim Sign" on contrast studies of the kidney is characteristically seen in which of the following conditions?
What is the X-ray appearance of a common bile duct stone on cholangiography?
What is the incidence of adrenal incidentaloma on CT scan?
What is the investigation of choice for recurrent GIST?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app