
Abdominal and Pelvic Radiology — MCQs

On this page
Which pattern on an abdominal radiograph is suggestive of intestinal obstruction?
Tear drop bladder is seen in which condition?
Gasless abdomen is a feature of which of the following conditions?
Which of the following is NOT a radiological sign of Crohn's disease?
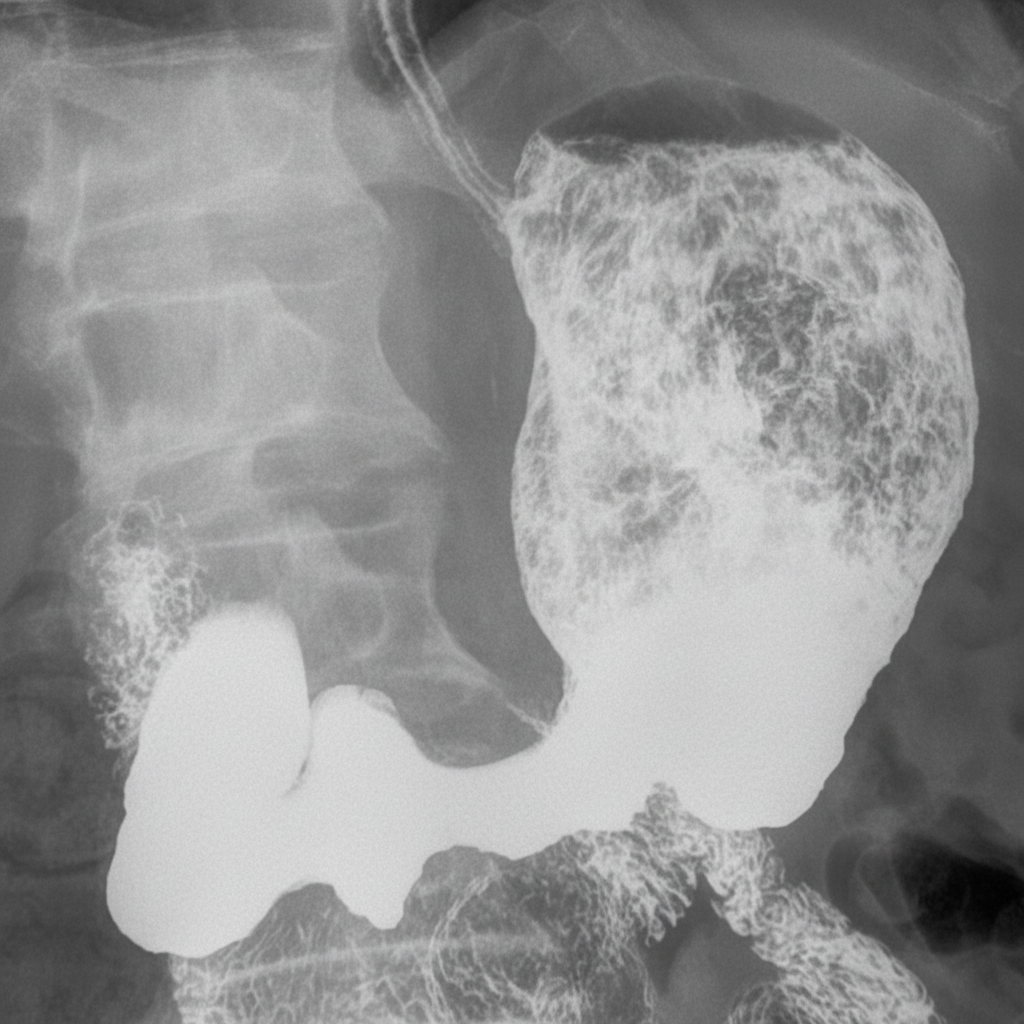
A 58-year-old man presents with epigastric discomfort, early satiety, peripheral edema, and unintentional weight loss. Laboratory testing shows hypoalbuminemia. The upper GI contrast study demonstrates markedly enlarged, tortuous cerebriform gastric folds involving predominantly the body and fundus, with relative sparing of the antrum. What is the most likely diagnosis?
The investigation of choice for imaging of urinary tract tuberculosis is:
A patient presents with mild abdominal pain and fluctuating bowel habits. The barium enema image is shown below. What is your diagnosis?

What is the characteristic 'crumbled egg appearance' in the liver associated with?
Colonic diverticulosis is best diagnosed by which imaging modality?
In case of suspected perforation, which radiological view is best?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app