
Abdominal and Pelvic Radiology — MCQs

On this page
Bosniak classification is used for the assessment of which of the following?
Spider leg appearance on intravenous urography is typically seen in which of the following conditions?
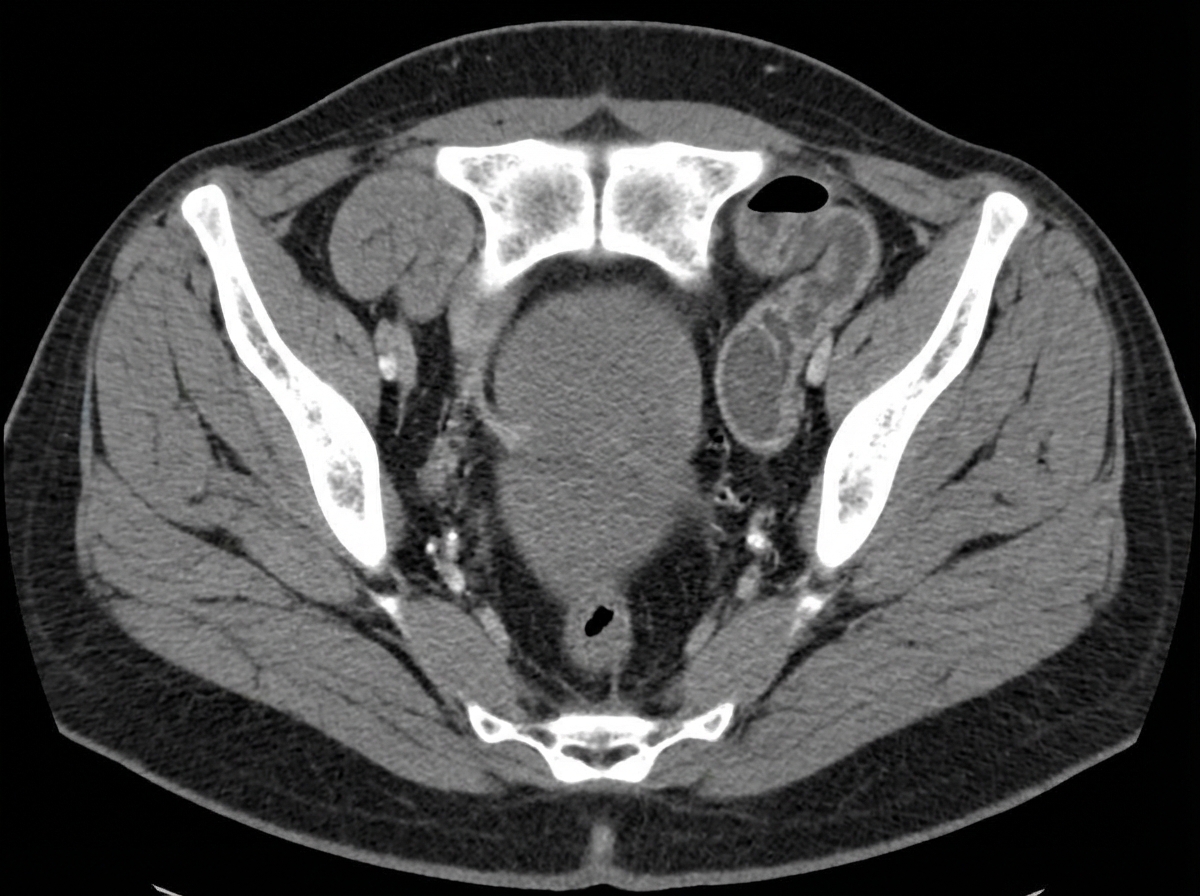
An elderly woman presented with abdominal pain and vomiting for three days. A computed tomogram of the abdomen was obtained. What is the diagnosis?
What is the most sensitive and specific investigation for screening of renovascular hypertension?
What is the gold standard investigation for renal artery stenosis in a 21-year-old girl?
Which of the following is the earliest sign of ulcerative colitis on a double contrast barium enema (DCBE) study?
A patient presents with marked loin pain, tenderness, and pyrexia. Initial investigations reveal non-specific findings on IVP. Ultrasound shows a heterogeneous mass with posterior acoustic enhancement and central necrosis and internal debris. CT scan demonstrates marginal enhancement with air densities within. What is the likely diagnosis?
Ultrasound and radionuclide studies are primary imaging modalities used for the assessment of which of the following conditions?
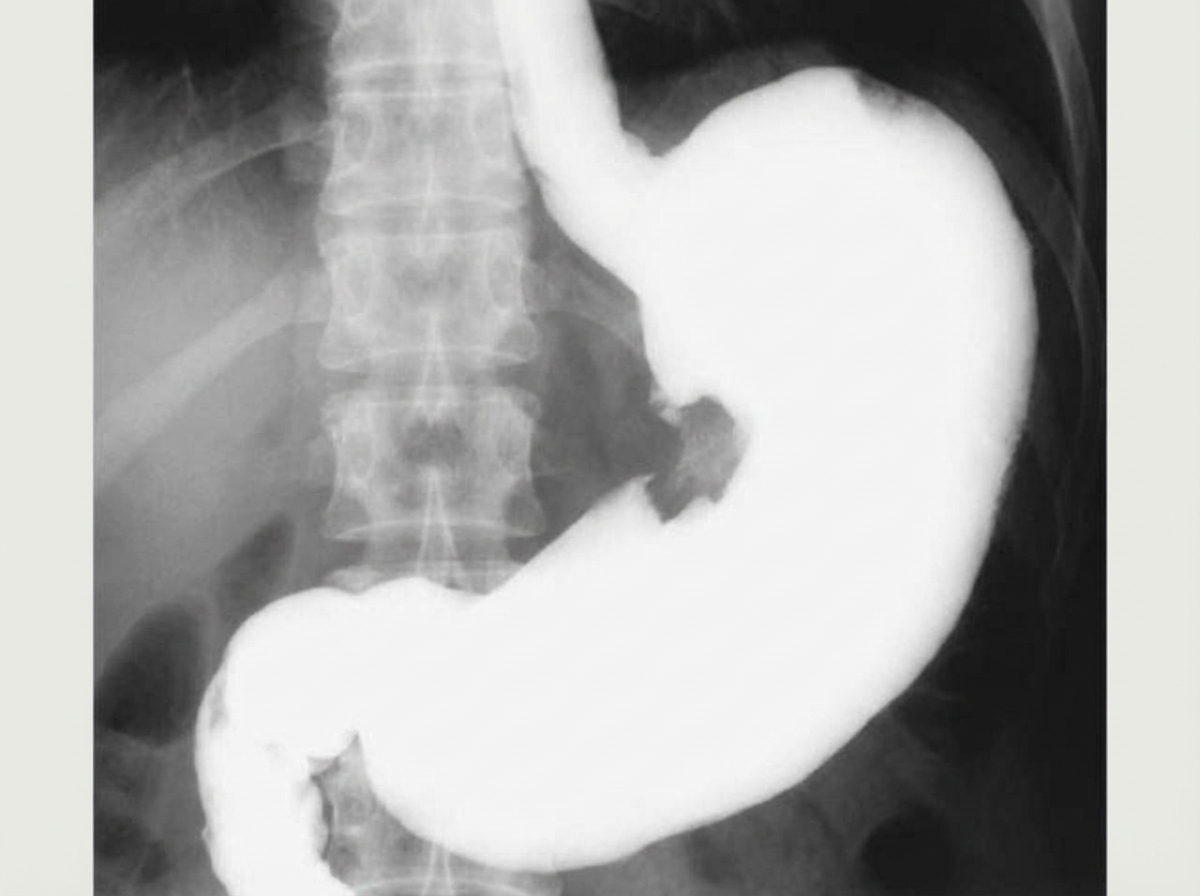
What is the principal radiographic abnormality seen in the contrast X-ray abdomen?
A DTPA scan of a hypertensive young lady is normal, and the USG shows a small left kidney. What is the next investigation?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app