
Abdominal and Pelvic Radiology — MCQs

On this page
What does 'pseudo kidney' refer to on ultrasound?
Ultrasonography of the liver shows a starry sky appearance. This is a feature of which condition?
Which of the following is NOT a diagnostic feature of gallstone ileus on a plain abdominal radiograph?
What is the most sensitive and specific investigation in renal artery hypertension?
Thickened gastric folds are found in which of the following conditions?
Which imaging modality is used for the initial assessment of acute pancreatitis?
The "collar button" sign is associated with which condition?
A 56-year-old male presents with burning micturition, increasing frequency, and hesitancy. An intravenous pyelogram was performed, and the radiograph is shown. What is the most likely diagnosis?
Which of the following is NOT a typical ultrasound finding of Autosomal Recessive Polycystic Kidney Disease (ARPKD)?
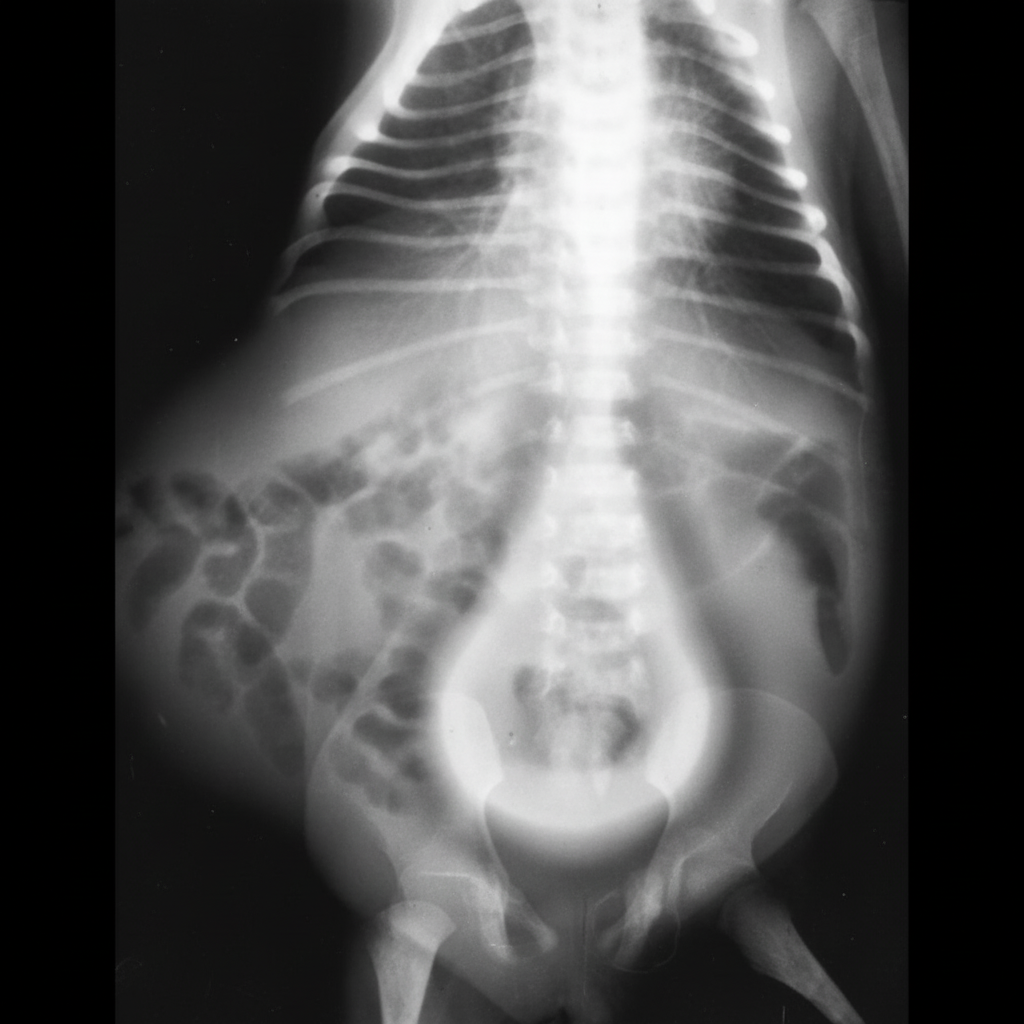
An X-ray of the abdomen shows multiple fluid levels. What is the most likely diagnosis?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app