
Abdominal and Pelvic Radiology — MCQs

On this page
The CT severity index is a measure for which of the following conditions?
In a high-risk population, hepatocellular carcinoma (HCC) is best detected by which imaging modality?
What is the investigation of choice for a small intestine tumor?
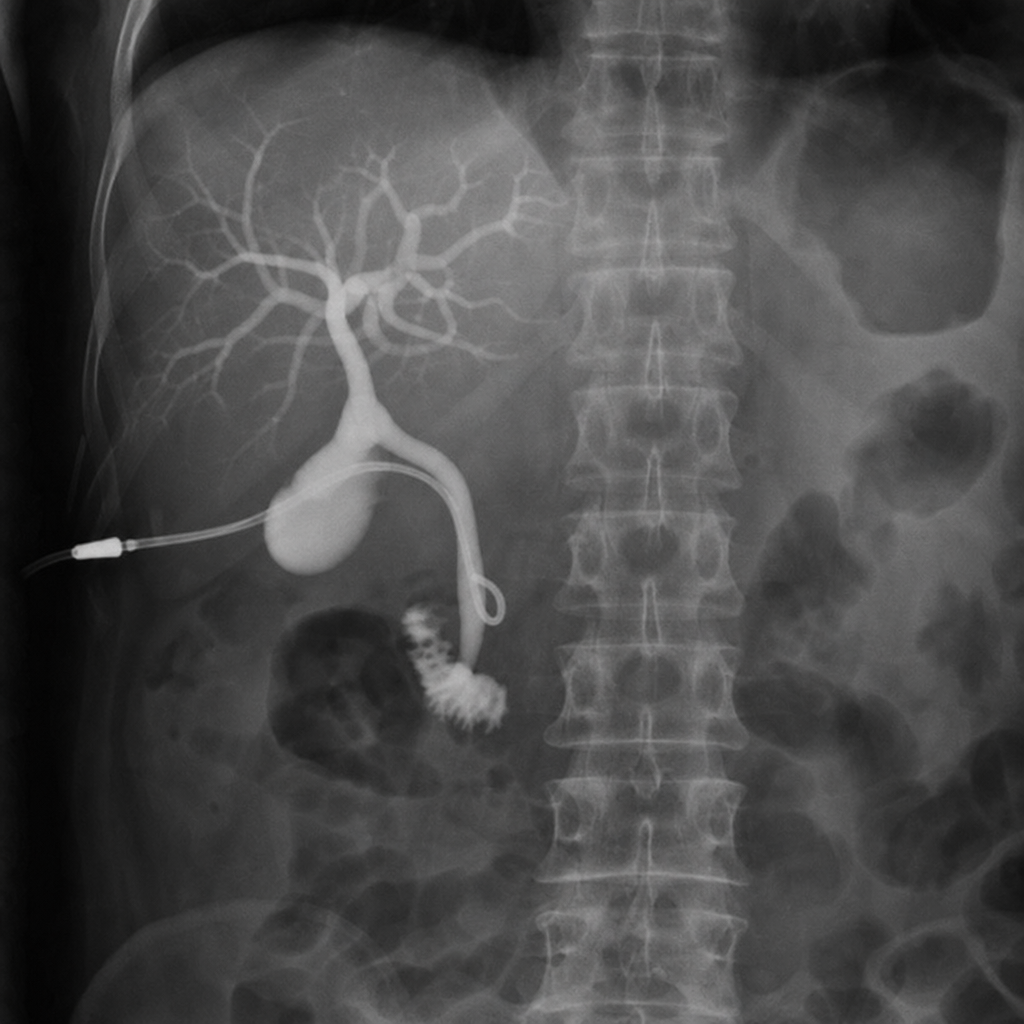
Which investigation is being performed?
What is a characteristic feature of the post-ovulatory endometrium observed on ultrasound?
Fleischner sign is characteristic of which condition?
Hyperchoice hepatic metastases on USG are seen in which of the following malignancies?
Which of the following is NOT a CT finding of acute pancreatitis?
Which of the following is NOT a radiological sign of Ulcerative colitis?
Which is the most important sign of significance of renal artery stenosis on an angiogram?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app