
Abdominal and Pelvic Radiology — MCQs

On this page
A patient presents with sudden severe epigastric pain and peritoneal signs. They have a known history of peptic ulcer disease. What is the diagnosis?
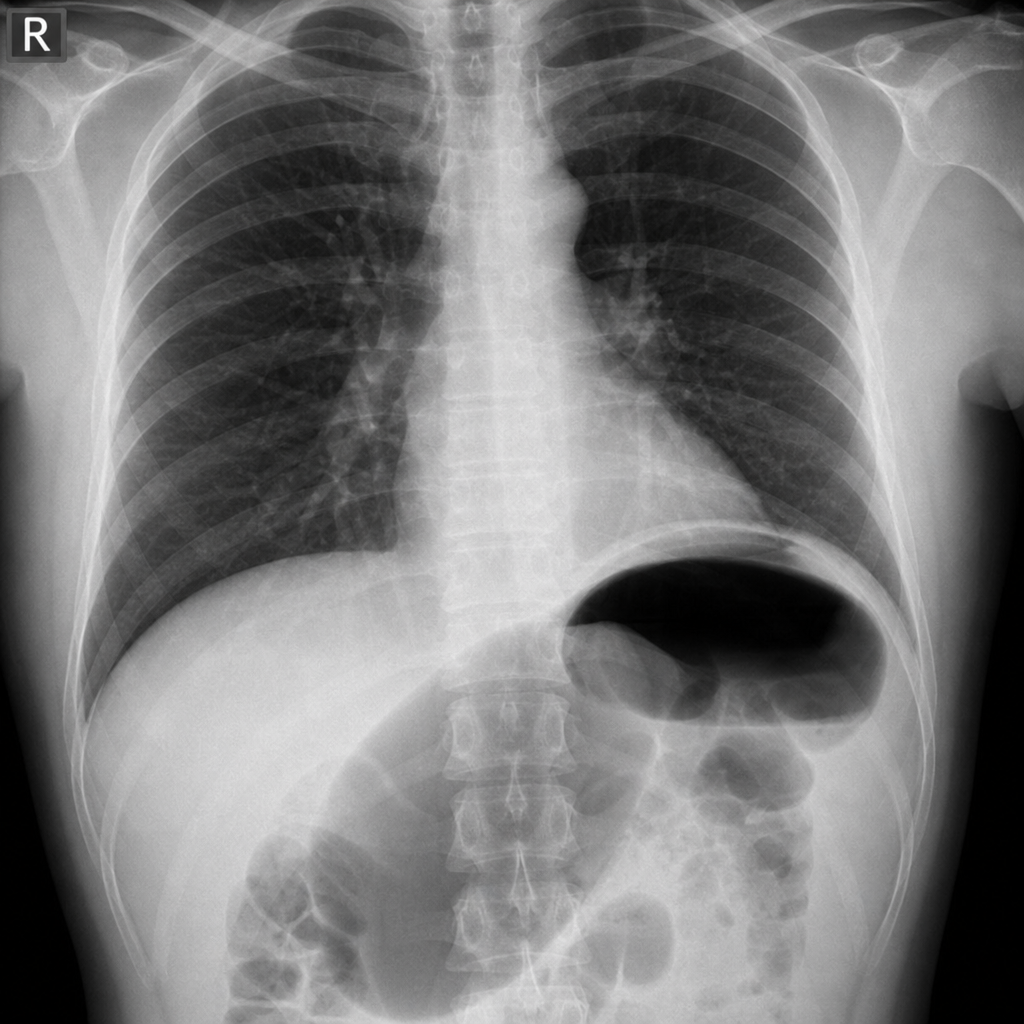
A 20-year-old male presents with multiple bruises on the anterior chest and abdominal regions. The attending surgeon suspects pneumoperitoneum and requests a chest X-ray. What is the best radiological view to detect pneumoperitoneum?
Information obtained by lateral plate X-ray pelvimetry includes all of the following EXCEPT:
Bear claw's sign is seen in which of the following conditions?
Medusa head appearance on abdominal X-ray indicates:
The 'Arrowhead Sign' on CT scan is a characteristic feature of which of the following conditions?
Which of the following is NOT a common feature of a malignant gastric ulcer on barium meal examination?
A hypoechoic lesion within the prostate is typically seen in which of the following conditions?
Frostburg's reverse 3 sign is seen in which of the following conditions?
Which investigation is done for intestinal obstruction?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app