
Abdominal and Pelvic Radiology — MCQs

On this page
Characteristic fallopian tube findings on sonography in pelvic inflammatory disease includes all except?
Which of the following investigations is NOT used for the diagnosis of renal stones?
Which of the following is an investigation for small intestine abnormalities, excluding one option?
A 54-year-old man presents with a 2-day history of mild abdominal pain, bloating, nausea, vomiting, and poor appetite. His past medical history is significant for recent pneumonia. Radiographic examination reveals a paralytic ileus. Which of the following signs would most likely be found during a physical examination?
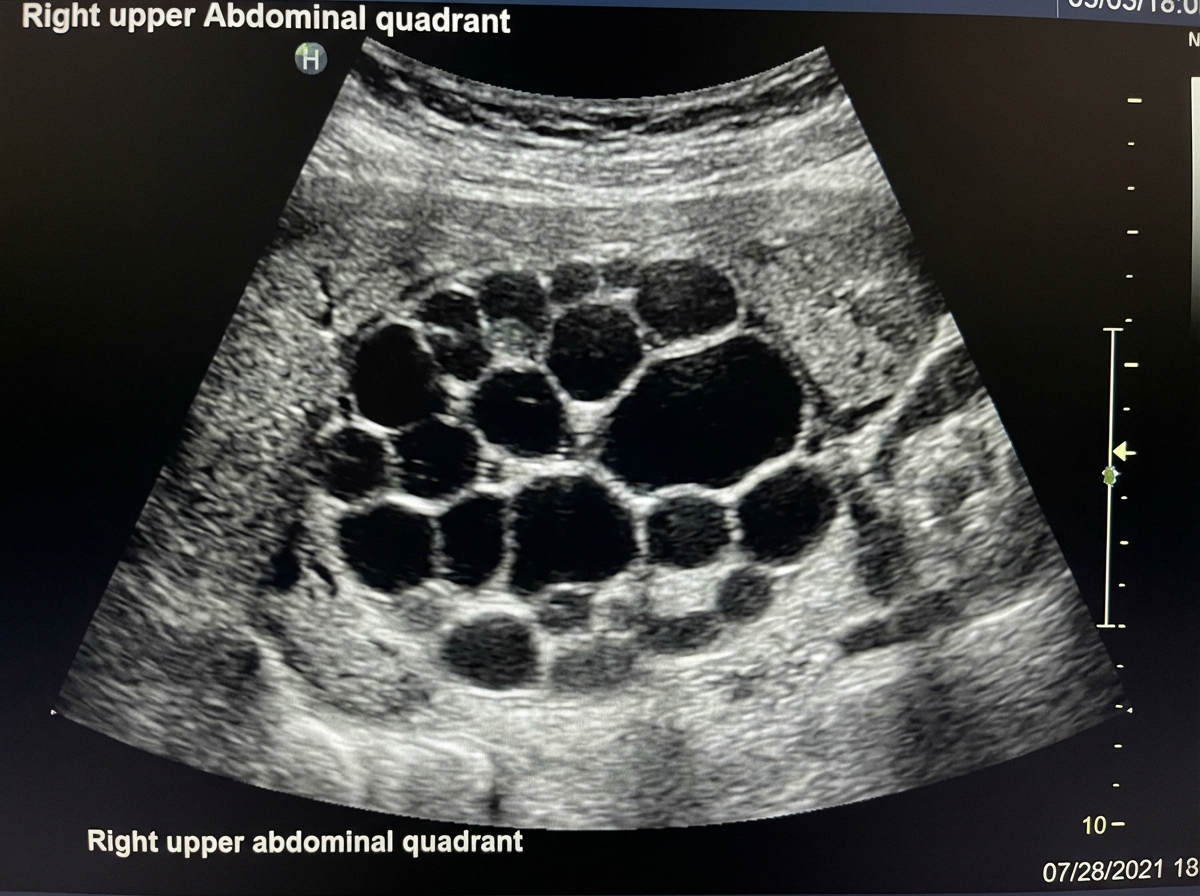
What is the type of Gharbi classification of the given hydatid cyst?
Barium esophagogram findings in carcinoma esophagus include all EXCEPT:
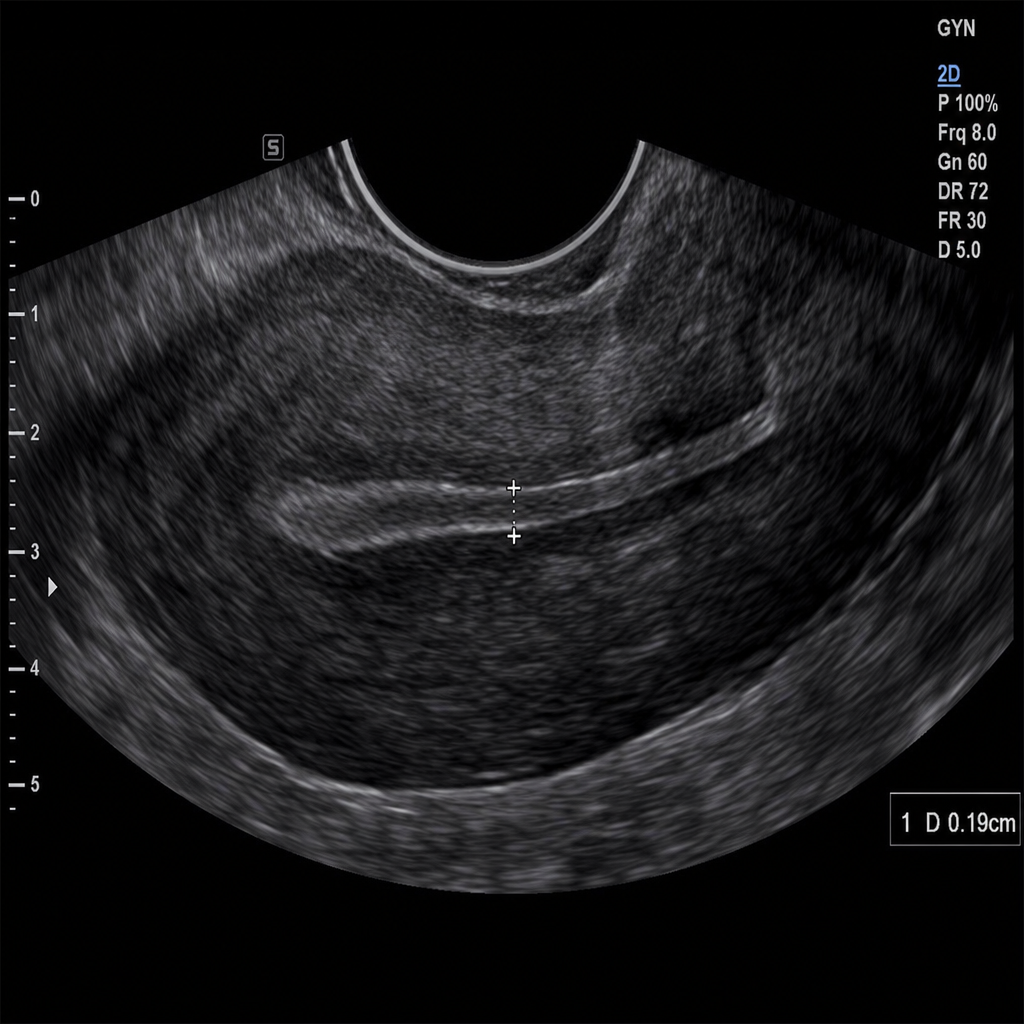
A TVS (Transvaginal Sonography) demonstrates which of the following endometrial findings?
Which area of the colon is least visualized by barium studies?
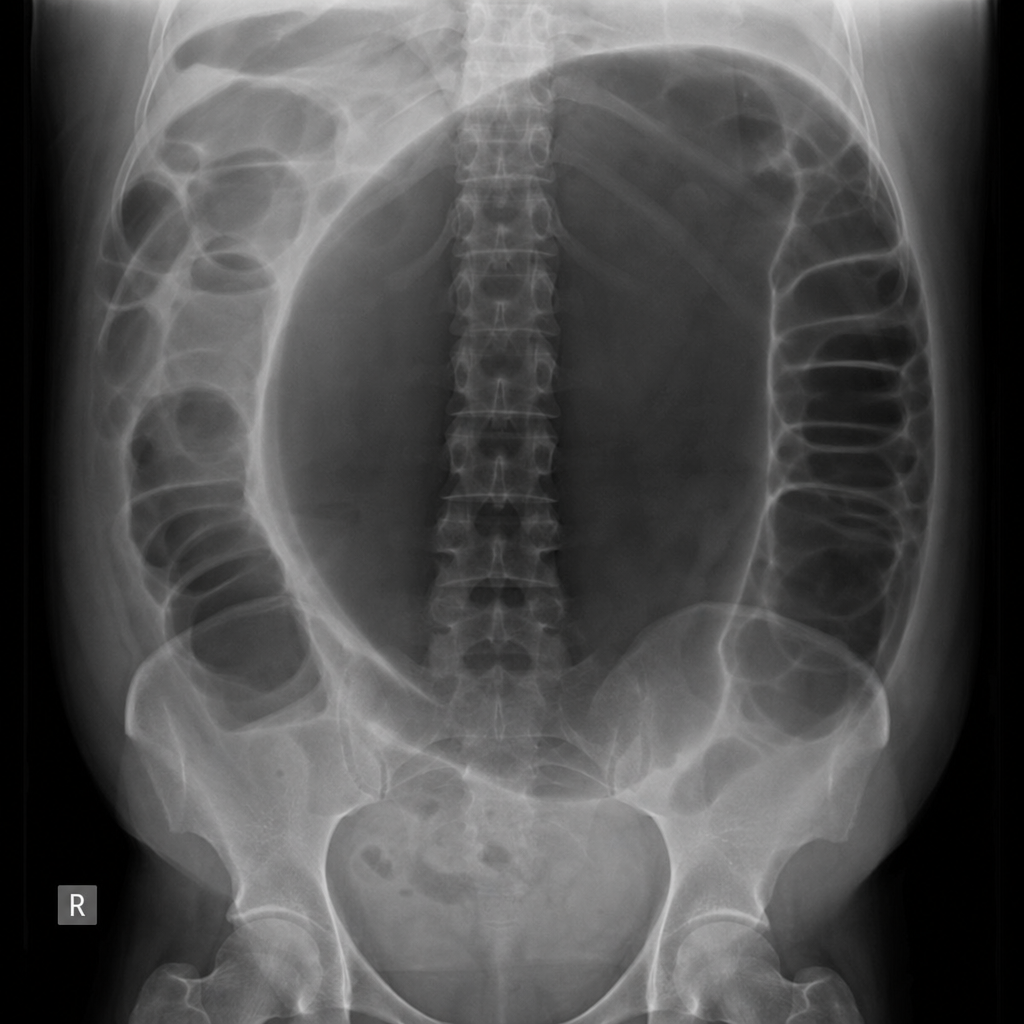
A patient presents with abdominal distension. X-ray of the patient is shown below. What is the probable diagnosis?
Pipe stem appearance in barium enema is characteristic of which condition?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app