
Abdominal and Pelvic Radiology — MCQs

On this page
A 40-year-old male presents with severe epigastric pain radiating to the back. On examination, his heart rate is 110/min, respiratory rate is 22/min, and blood pressure is 100/70 mmHg. His abdominal X-ray is shown below. What does the X-ray depict?

What is the diagnosis suggested by the barium study film?

Renal tuberculosis can be diagnosed earliest by which imaging modality?
What is the most common cause of 'target lesion' in the stomach?
The Seagull sign is seen in which of the following conditions?
What is the diagnosis suggested by the provided X-ray of the abdomen?

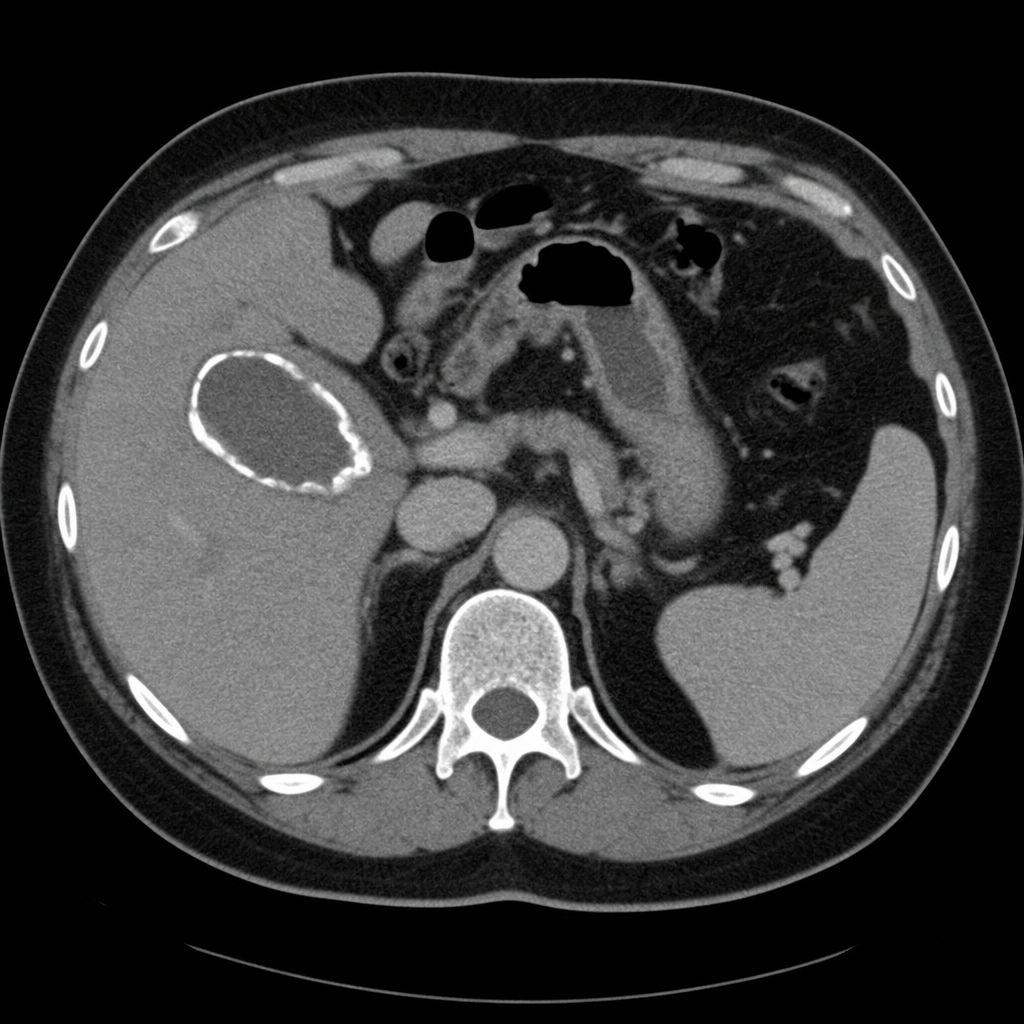
An incidental finding in a 56-year-old female patient who underwent CECT abdomen is suggestive of which of the following?
Which type of mesenteric ischemia is best visualized by CECT?
Parallel shotgun appearance on Ultrasound is seen in which of the following conditions?
What is the most sensitive investigation for pancreatic carcinoma?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app