
Abdominal and Pelvic Radiology — MCQs

On this page
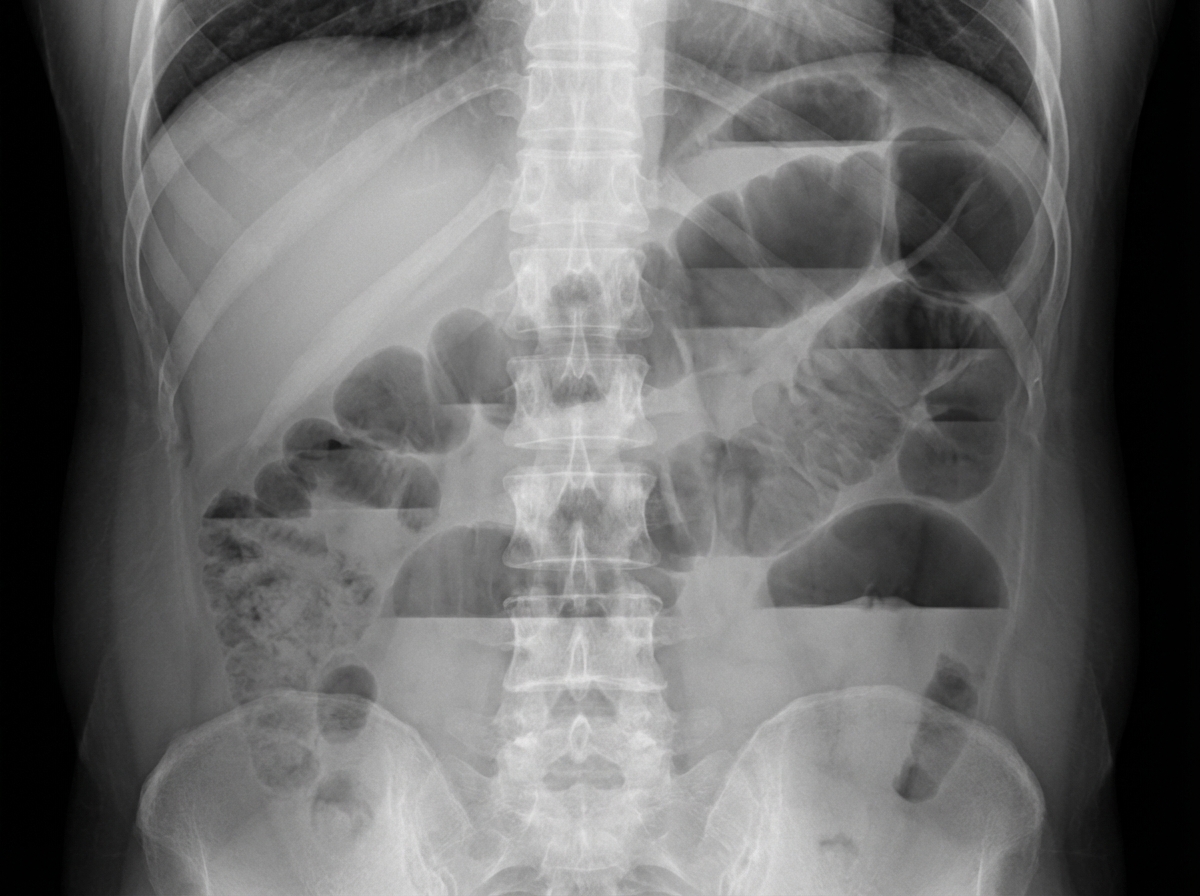
Which of the following is the most probable diagnosis based on the provided X-ray of the abdomen?
The 'spider leg' sign on an intravenous pyelogram (IVP) suggests which of the following conditions?
Diagnose the uterine condition shown on hysterosalpingogram.

A linear filling defect on ERCP is characteristic of which of the following conditions?
The endometrium during the proliferative phase appears as all except:
Which of the following is NOT a radiological sign of uterine fibroid?
Spider leg deformity of calyces on IVP is seen in which of the following conditions?
Gas under the diaphragm is seen in which of the following conditions?
Claw sign or pincer sign is seen in which of the following conditions?
Which imaging modality is considered the gold standard for diagnosing Crohn's disease?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app