
Abdominal and Pelvic Radiology — MCQs

On this page
What is the investigation of choice for retroperitoneal soft tissue sarcomas?
A previously healthy 61-year-old woman presents with a 3-week history of altered bowel habit and rectal bleeding. She refuses to undergo colonoscopy. Which of the following is the next best investigation?
A 40-year-old male complains of recurrent urinary tract infections. An X-ray KUB shows a radio-opaque shadow. What is the most likely diagnosis?
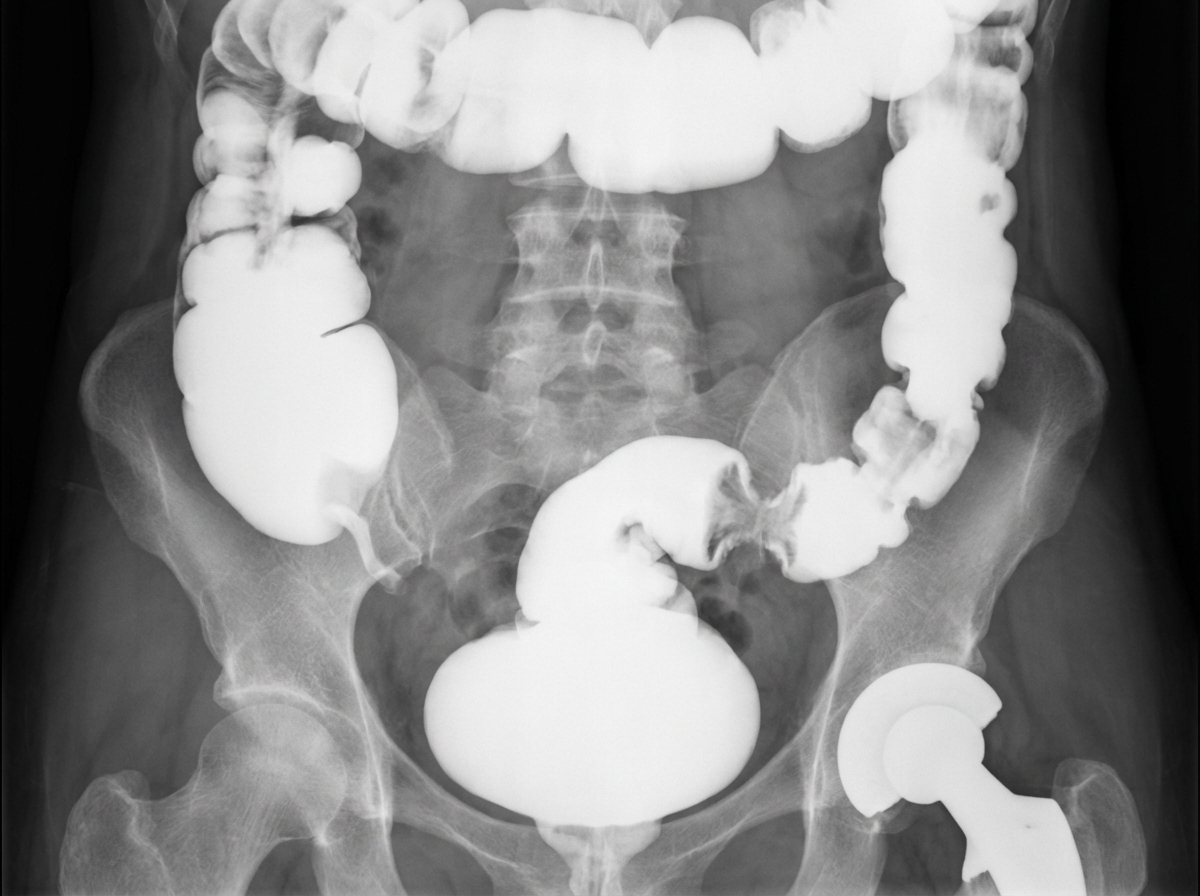
A contrast enema in this 82-year-old patient with diabetes mellitus who had undergone a total hip replacement 10 years previously demonstrates passage of contrast into the urinary bladder. What is the most likely underlying diagnosis responsible for this finding?
What do the arrows on an abdominal radiograph indicate?
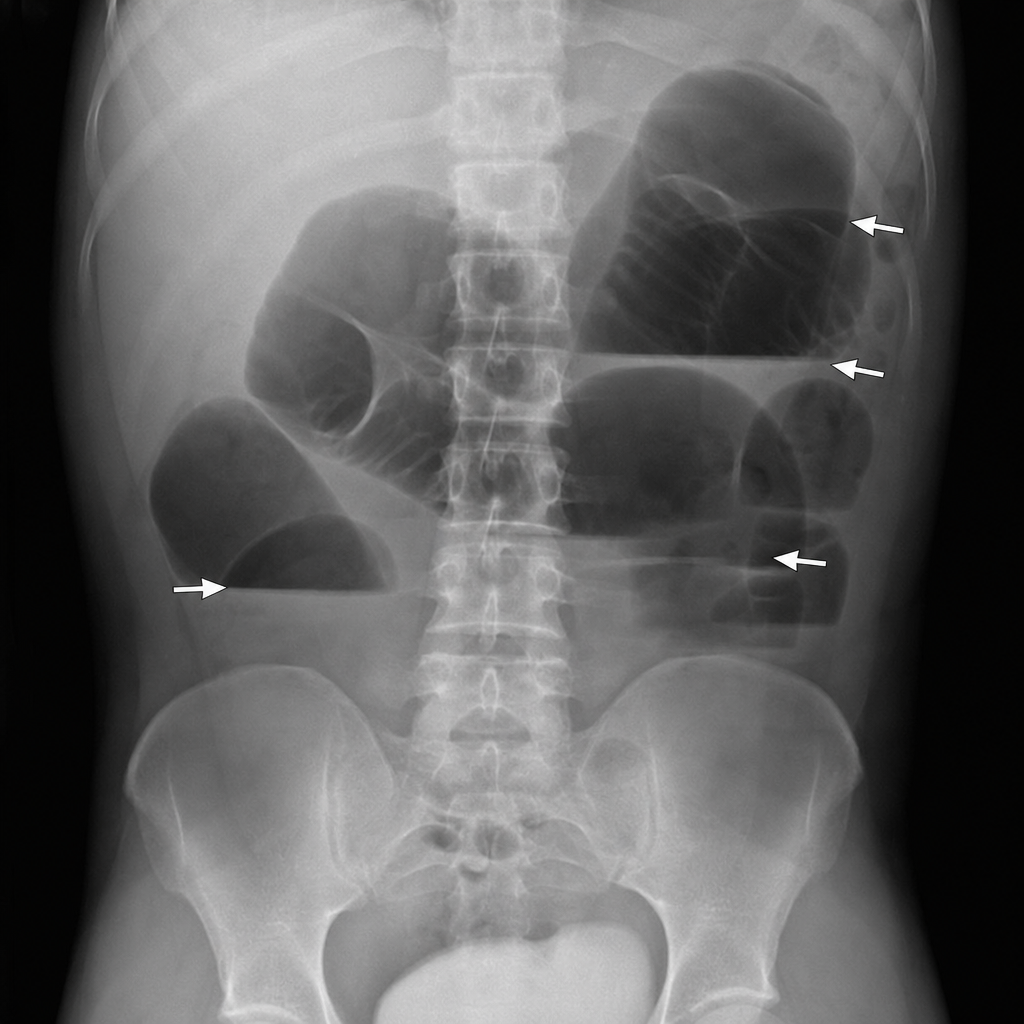
All are true about the radiological features of intestinal obstruction except?
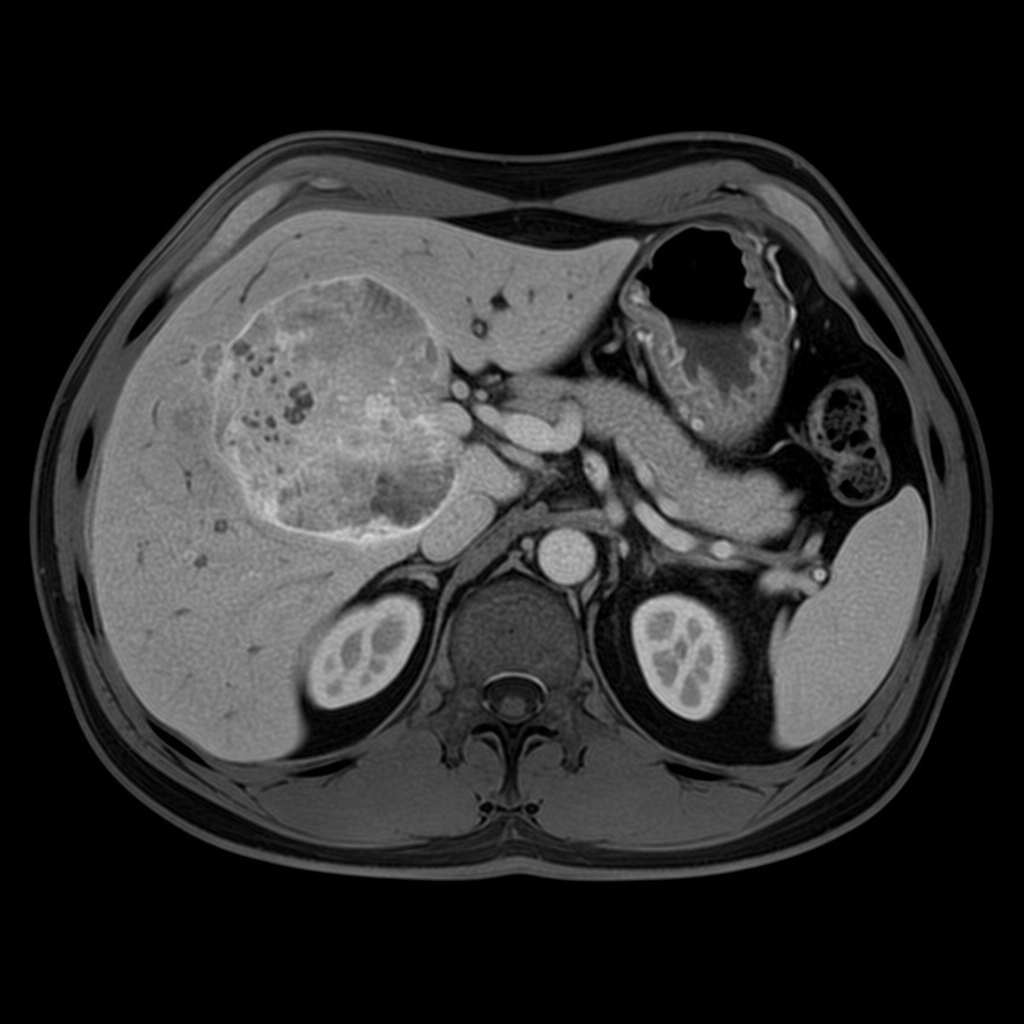
A 45-year-old patient is found to have an incidental adrenal mass on routine imaging. The lesion is shown above. Which MRI sequence is best suited for characterizing this adrenal lesion?
The "string sign" on imaging is suggestive of which of the following conditions?
A middle-aged patient presents with a complaint of right hypochondrial pain. An X-ray shows an elevated right hemidiaphragm. Which of the following is NOT a possible diagnosis?
Thumb printing on imaging is characteristic of which of the following conditions?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app