
Abdominal and Pelvic Radiology — MCQs

On this page
Which is the commonest incidentaloma detected in the liver?
What is the most sensitive test for ureteric stones?
What is the investigation of choice for testicular swelling?
What is the earliest radiological finding of Crohn's disease?
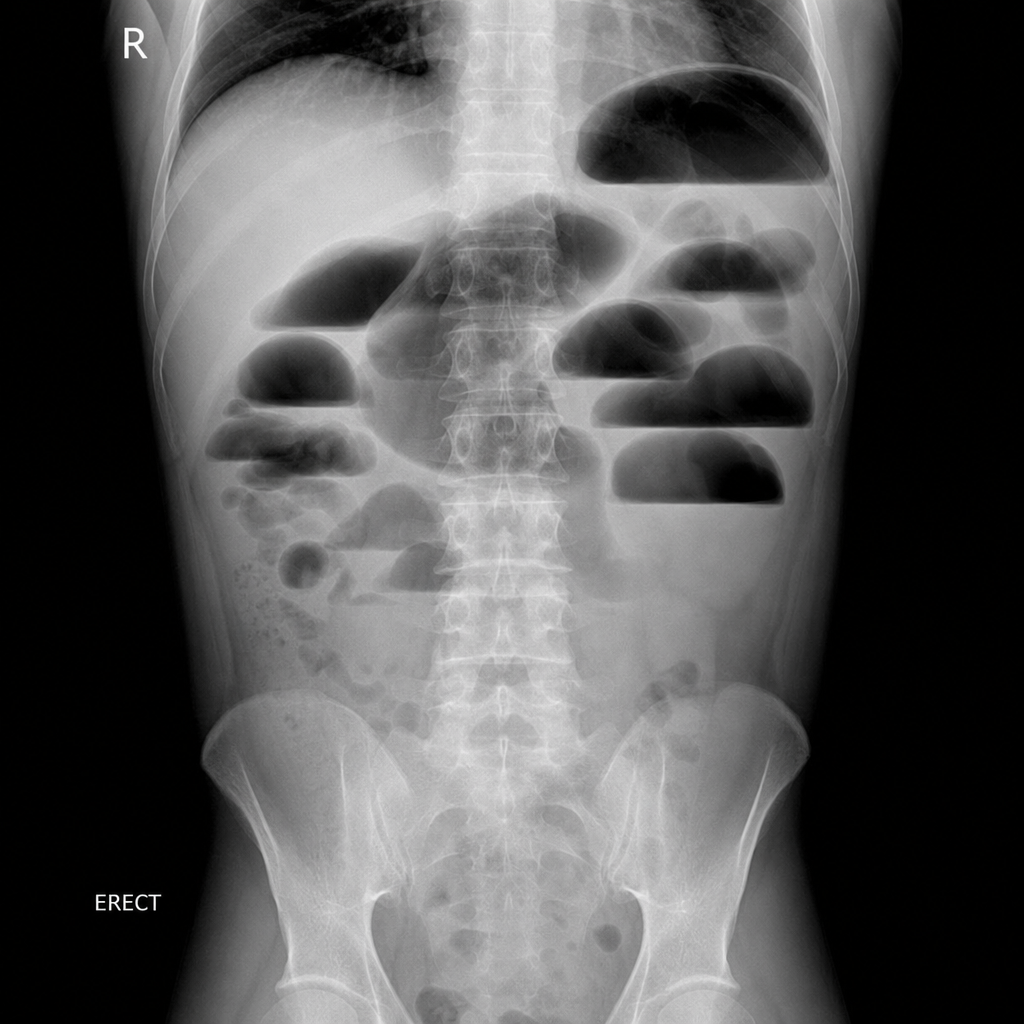
An X-ray showing intestinal obstruction is presented. Which view is depicted?
A patient presents with severe right upper quadrant pain associated with nausea and vomiting, exacerbation during inspiration, and tenderness on palpation. Which of the following imaging modalities is the investigation of choice for this patient?
For hiatus hernia, what is the investigation of choice?
The triad of pelvic lipomatosis includes all of the following except?
What type of CT scan is used to characterize the chemical composition of kidney stones?
What is the investigation of choice for a pregnant lady presenting with an upper abdominal mass?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app