
Abdominal and Pelvic Radiology — MCQs

On this page
What condition is characterized by an "upside down" stomach appearance on a Barium meal study?
Elevation of which of the following metabolites in Magnetic Resonance Spectroscopy suggests a possibility of carcinoma of the prostate?
A 28-year-old male presents with sudden onset of severe, colicky right lower abdominal pain. Ultrasound KUB showed mild hydronephrosis of the right kidney but no evidence of stones. Renal function tests and creatinine levels were normal. Urine culture was negative. What is the most appropriate next step?
Which of the following is NOT a radiological sign of acute pancreatitis?
Scrambled egg appearance is seen in which of the following conditions?
The 'drooping water lily' sign is seen in which of the following conditions?
The "mushroom cap sign" in MRI is most commonly seen in which of the following conditions?
Gas shadow in the heart and vessels is seen in which condition?
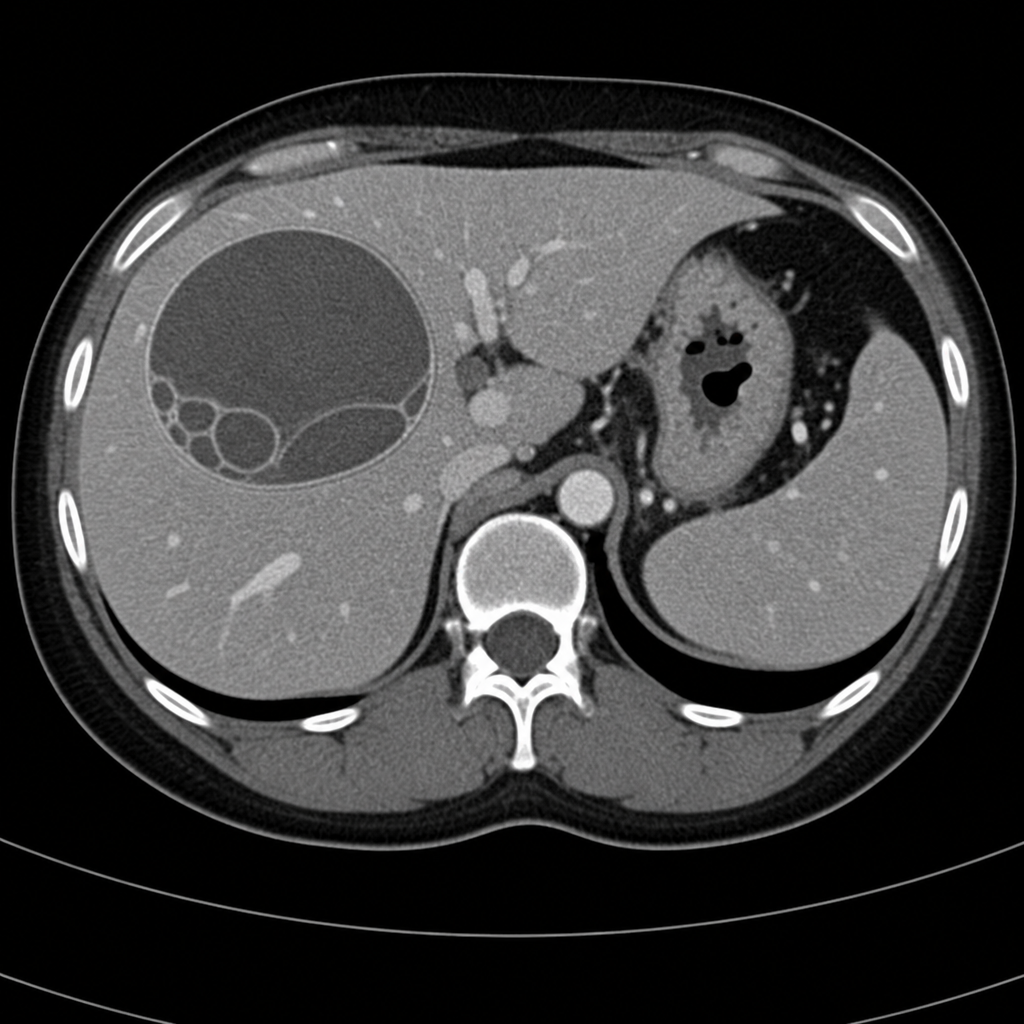
A middle-aged female presents with chronic right-sided abdominal pain and intermittent fever. Clinical examination revealed mild hepatomegaly. A contrast-enhanced CT abdomen was performed. Based on the imaging characteristics of the focal lesion, what is the most likely diagnosis?
Spot the diagnosis in the following IVU image?

Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app