
Abdominal and Pelvic Radiology — MCQs

On this page
What is the best diagnostic method for pancreatic cancer?
A 72-year-old man is found on examination to have a prostatic nodule. What is the best investigation to evaluate this finding?
The stipple sign in transitional cell carcinoma of the renal collecting system is best demonstrated by which imaging modality?
Radiologically, how is a small intestine distinguished from a large intestine in cases of intestinal obstruction?
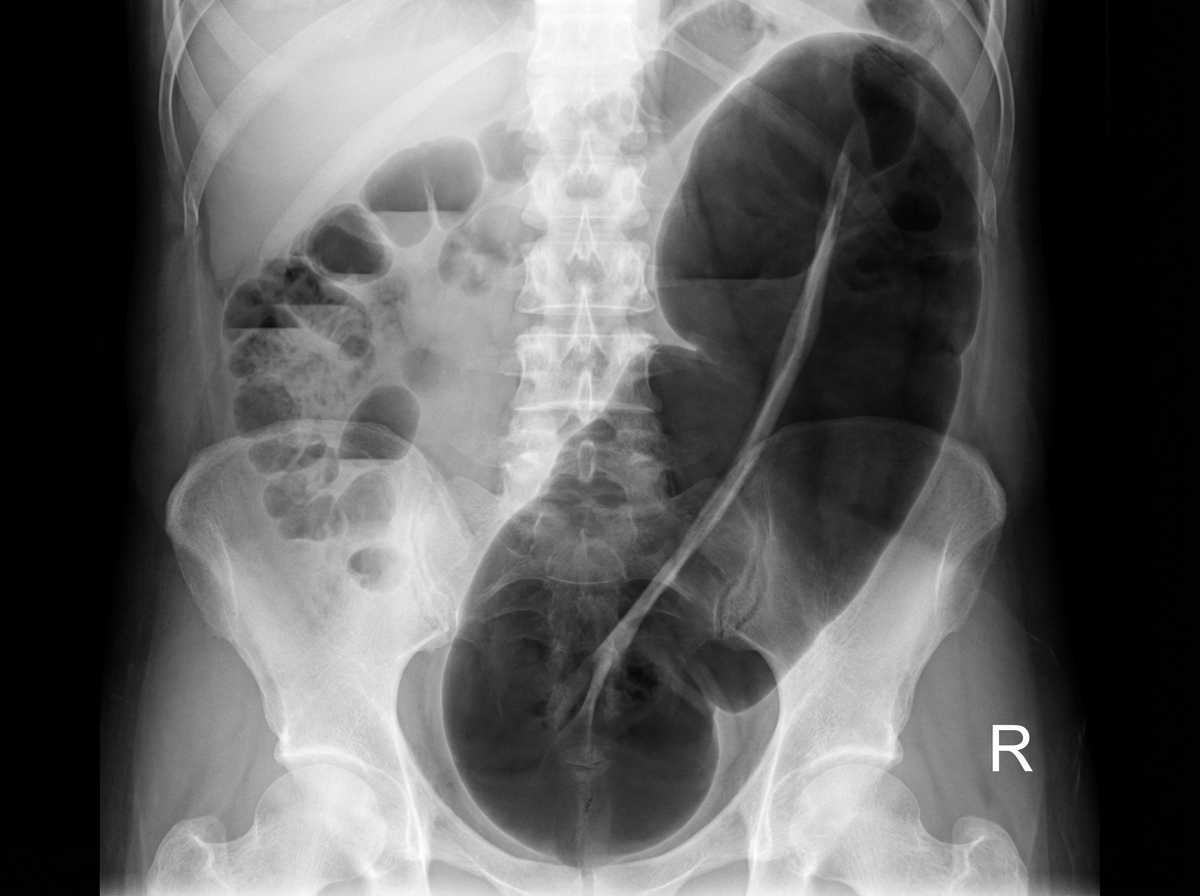
An X-ray of the abdomen reveals a specific finding. Identify the finding and its associated pathology:
What is the investigation of choice to evaluate the inferior vena cava and renal vein for thrombus in a patient with renal cell carcinoma?
Which of the following is NOT a radiological sign of pneumoperitoneum?
Thickened gall bladder wall in USG is seen in which of the following conditions?
The "fat ring sign" is characteristic of which condition?
Delayed centripetal contrast enhancement pattern is seen in which of the following conditions?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app