
Abdominal and Pelvic Radiology — MCQs

On this page
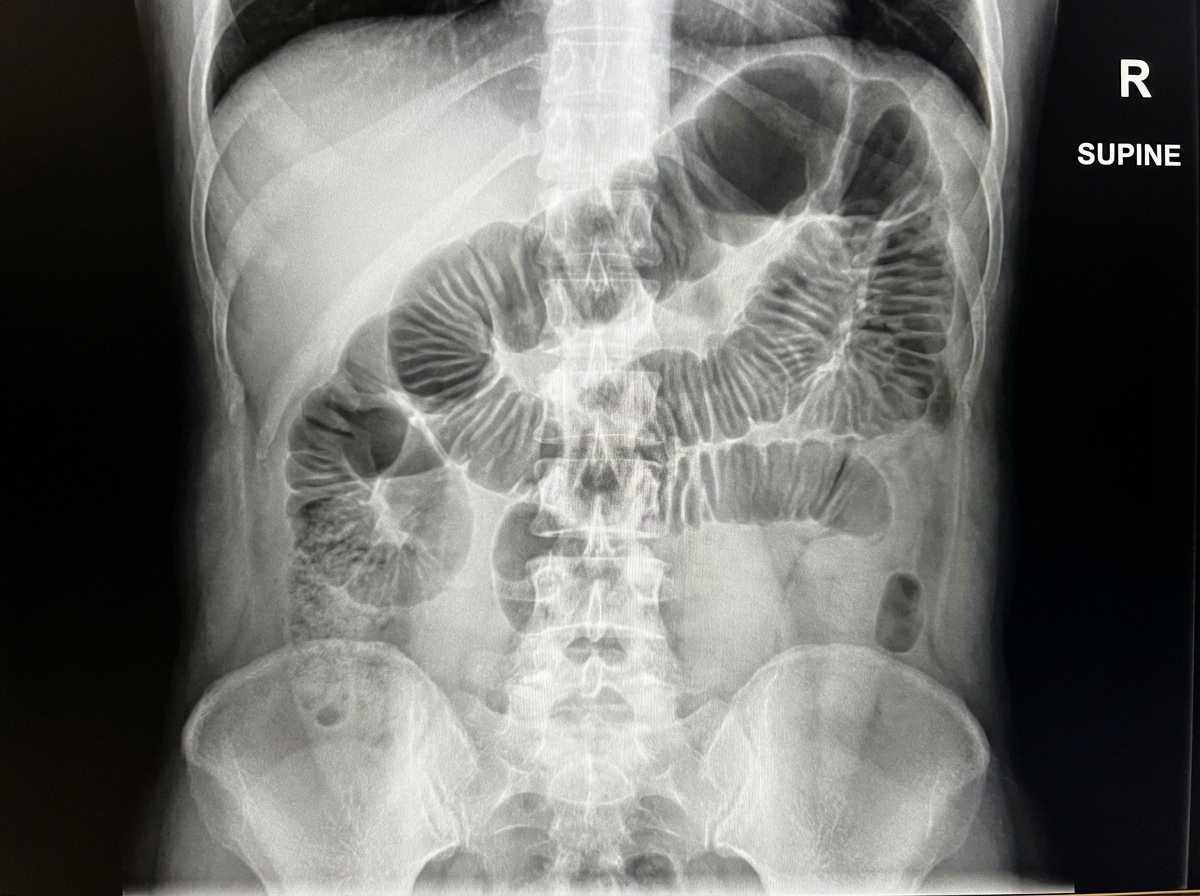
A sentinel loop is seen on an X-ray. What is the most likely diagnosis?
Which of the following is NOT a feature of Ulcerative Colitis?
Which ultrasonographic finding is characteristic of a hydatidiform mole?
The 'pencil tip' deformity is typically observed in which of the following conditions?
Which of the following is NOT a feature of chronic pancreatitis associated with pancreatic cancer?
Multiphasic hepatic imaging includes all except?
What is a potential limitation of Contrast-Enhanced Computed Tomography (CECT) in the evaluation of acute pancreatitis?
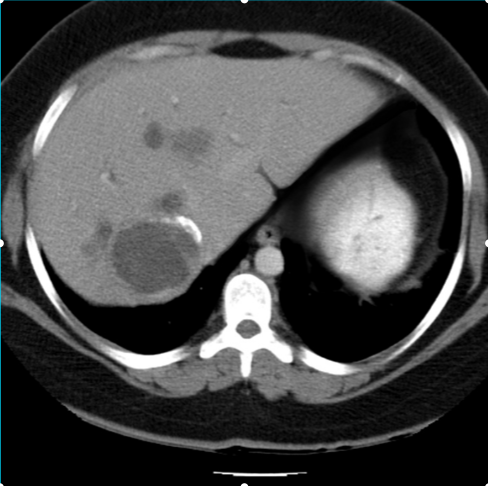
A middle-aged female presents with chronic right-sided abdominal pain and intermittent fever. Clinical examination reveals mild hepatomegaly. A contrast-enhanced CT abdomen was performed. Based on the imaging characteristics of the focal lesion, what is the most likely diagnosis?
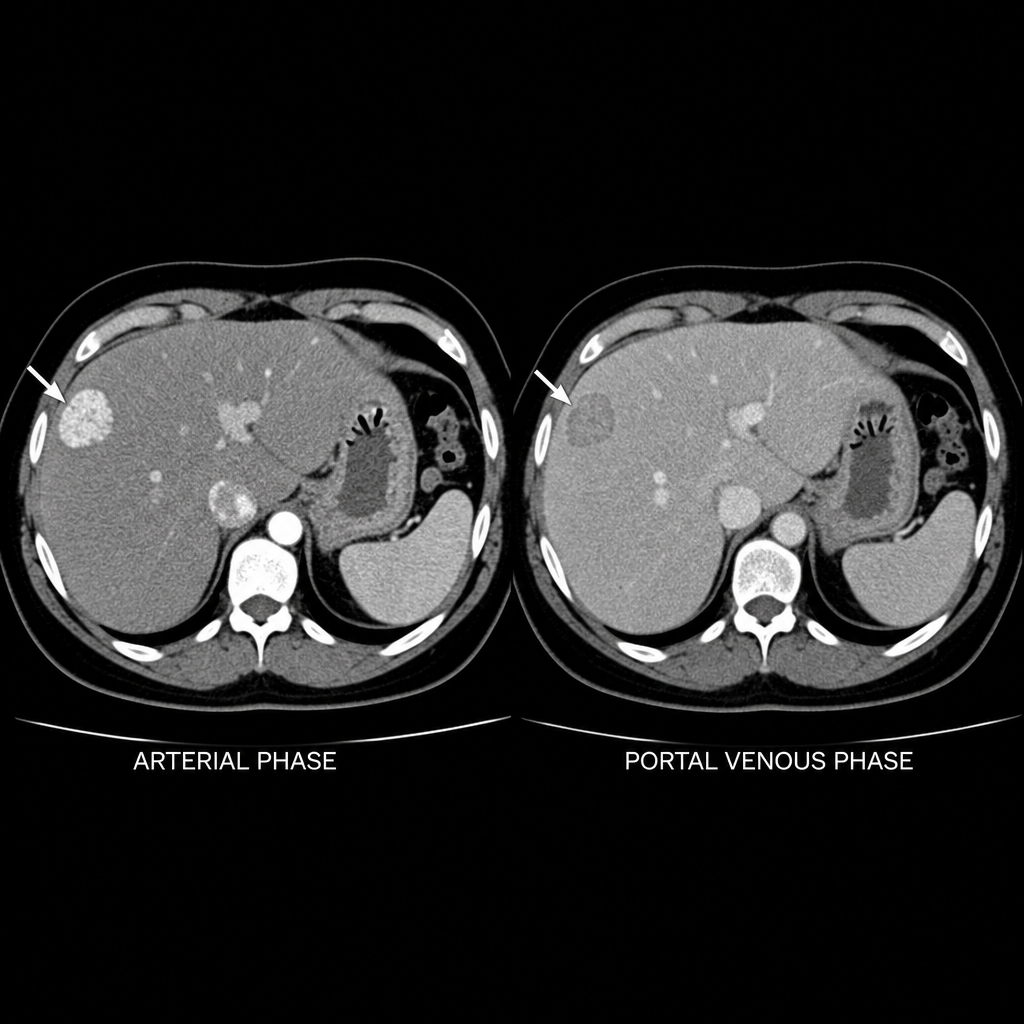
A young woman on oral contraceptives with no history of liver disease presents for abdominal imaging. The liver lesion pointed out with the arrow (CT - arterial and 10-minute delayed phases) is most likely to be?
The X-ray demonstrates which of the following conditions?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app