
Abdominal and Pelvic Radiology — MCQs

On this page
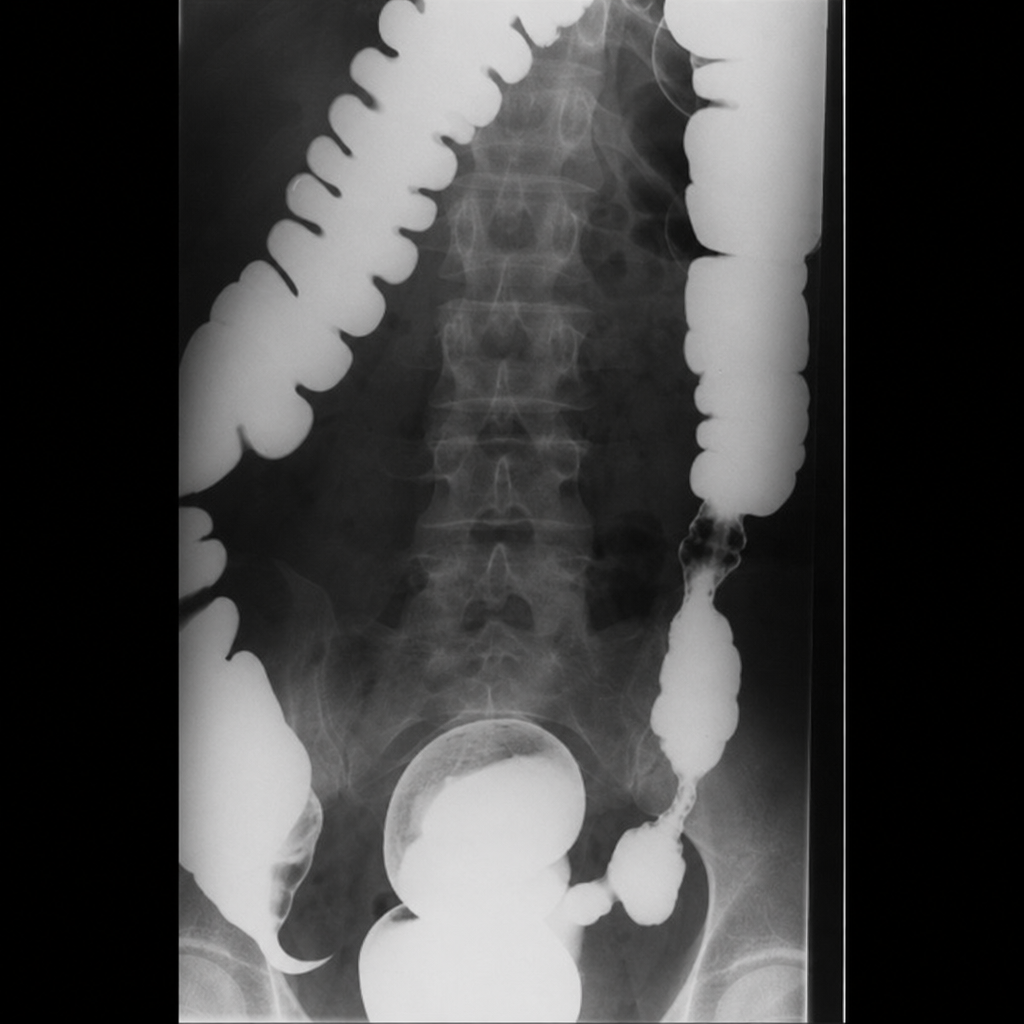
A barium enema examination is suggestive of which of the following findings?
What percentage of gallstones are radio-opaque?
Snow storm ascites is seen in which of the following conditions?
What is the investigation of choice to visualize the gallbladder?
In the suppurative phase, a pyogenic liver abscess will appear as what on ultrasound?
What is a typical ultrasound finding in chronic renal disease?
Which of the following is not a feature of renovascular hypertension on IVU?
A plain X-ray abdomen is performed in a case of small bowel obstruction. Small bowel is considered dilated if its diameter is more than:
Which of the following is NOT true regarding a renal pseudotumor?
'Thumb print' appearance on Barium enema is found in:
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app