
Abdominal and Pelvic Radiology — MCQs

On this page
Radiography of which of the following renal stones shows opacity, EXCEPT?
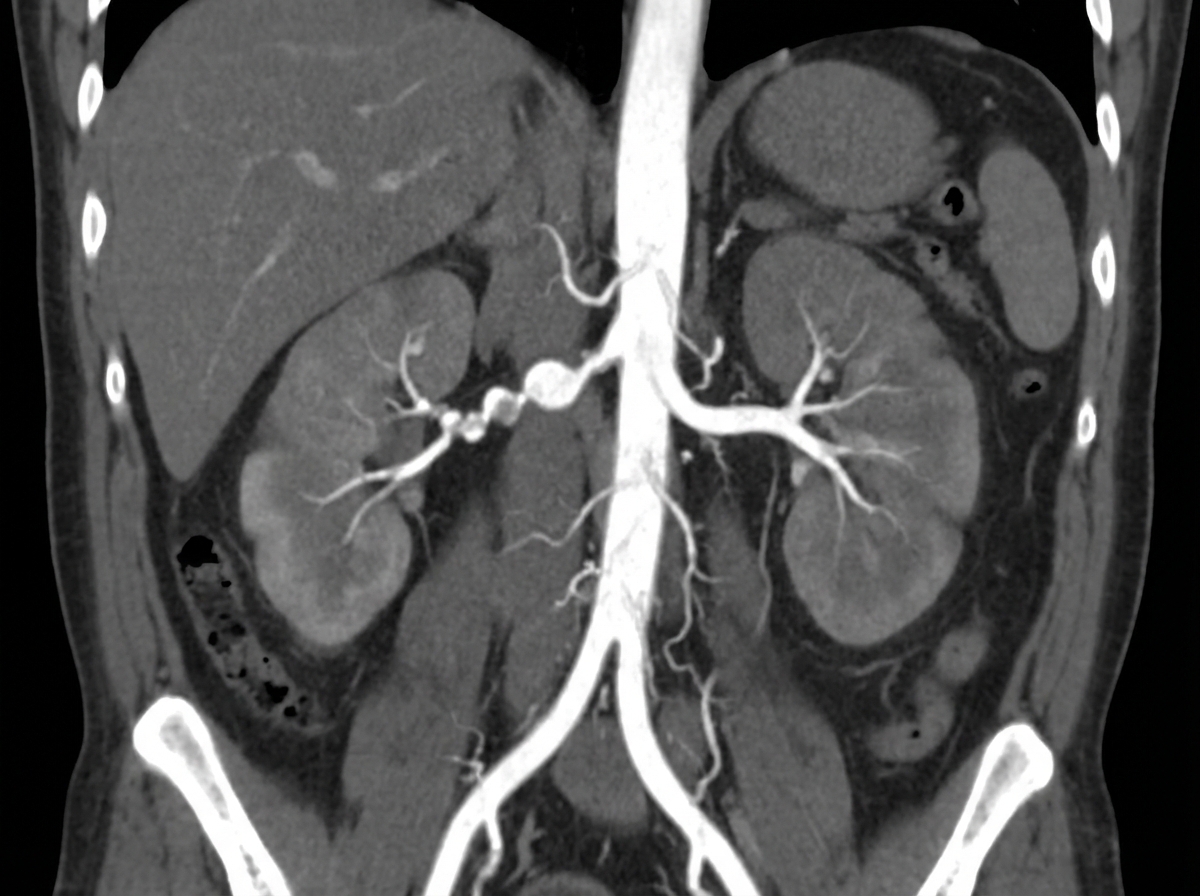
A 26-year-old male presents with abdominal pain and episodes of hematuria. His blood pressure is 160/100 mm Hg and is refractory to standard antihypertensive drugs. Renal Doppler shows a parvus tardus pattern. Subsequent CT renal angiogram was performed. Renal artery stenosis causing renovascular hypertension may occur in all of the following except?
Which of the following is NOT a feature of ischemic colitis?
The most appropriate investigation for diagnosing the condition shown in the X-ray is:

Confluent areas of pancreatic parenchyma that do not demonstrate enhancement after the administration of intravenous contrast material are known as?
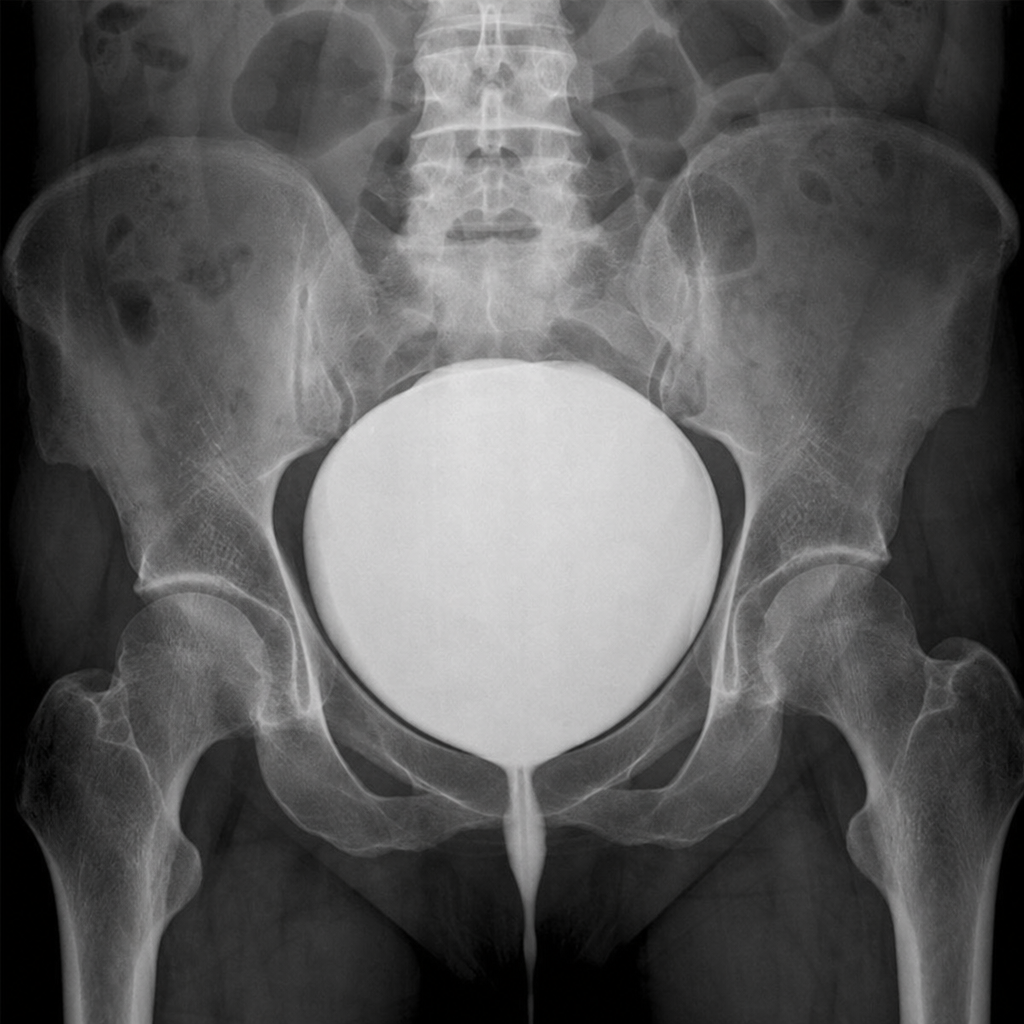
Which of the following is most likely to cause the given cystogram appearance?
Which of the following is NOT a feature suggestive of acute cholecystitis on CT abdomen?
A large volume of gas is seen at the subdiaphragmatic level on an X-ray. What is the most likely diagnosis?
What is the characteristic finding of a "saw tooth appearance" in an abdominal barium enema X-ray?
CT findings in gastric volvulus typically include which of the following?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app