
Abdominal and Pelvic Radiology — MCQs

On this page
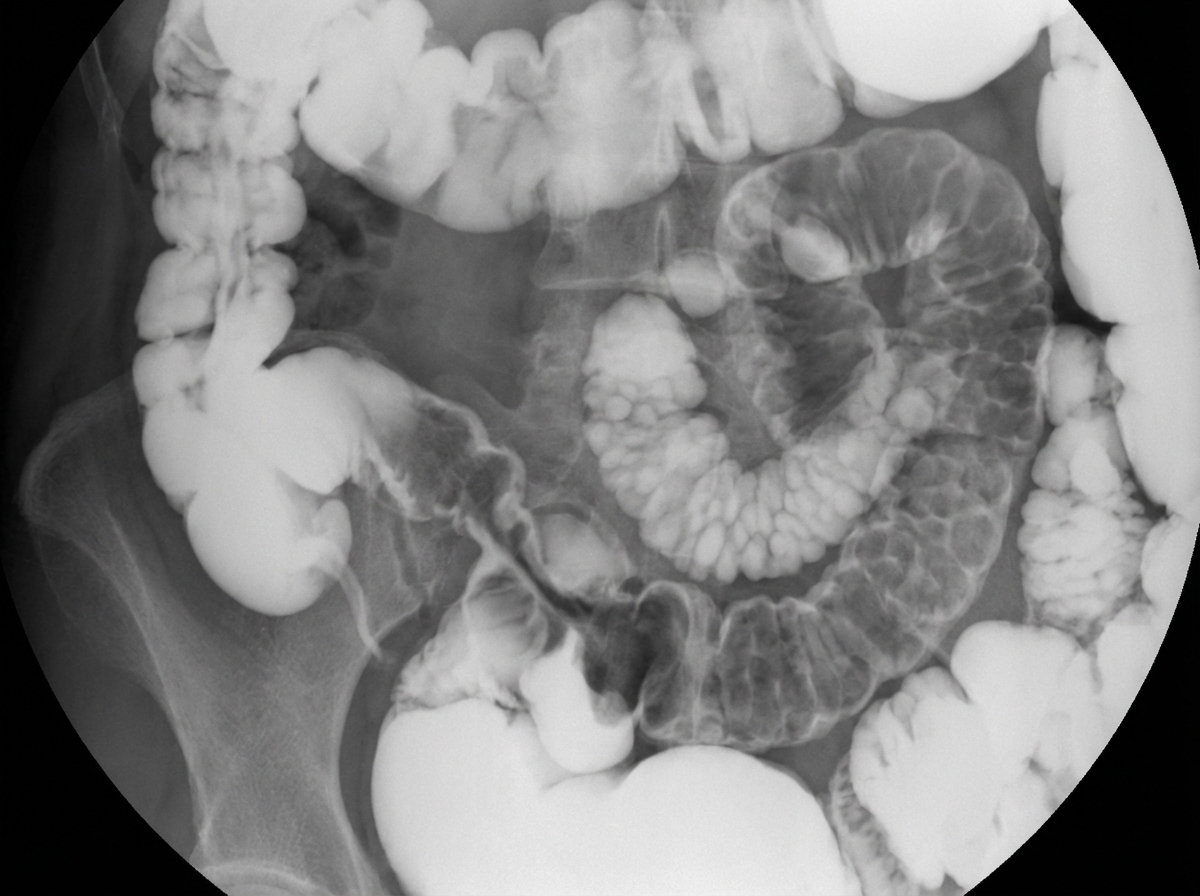
What is the most probable diagnosis on this barium film?
What is the most important use of transrectal ultrasonography (TRUS)?
An adult male presented with abdominal pain and diarrhea. A Barium meal follow-through revealed a mildly narrowed lumen of a loop with stretched and fixed rigid walls. A CT contrast study showed a stellate-shaped, enhancing mesenteric lesion with adjacent bowel wall thickening. What does this mass lesion represent?
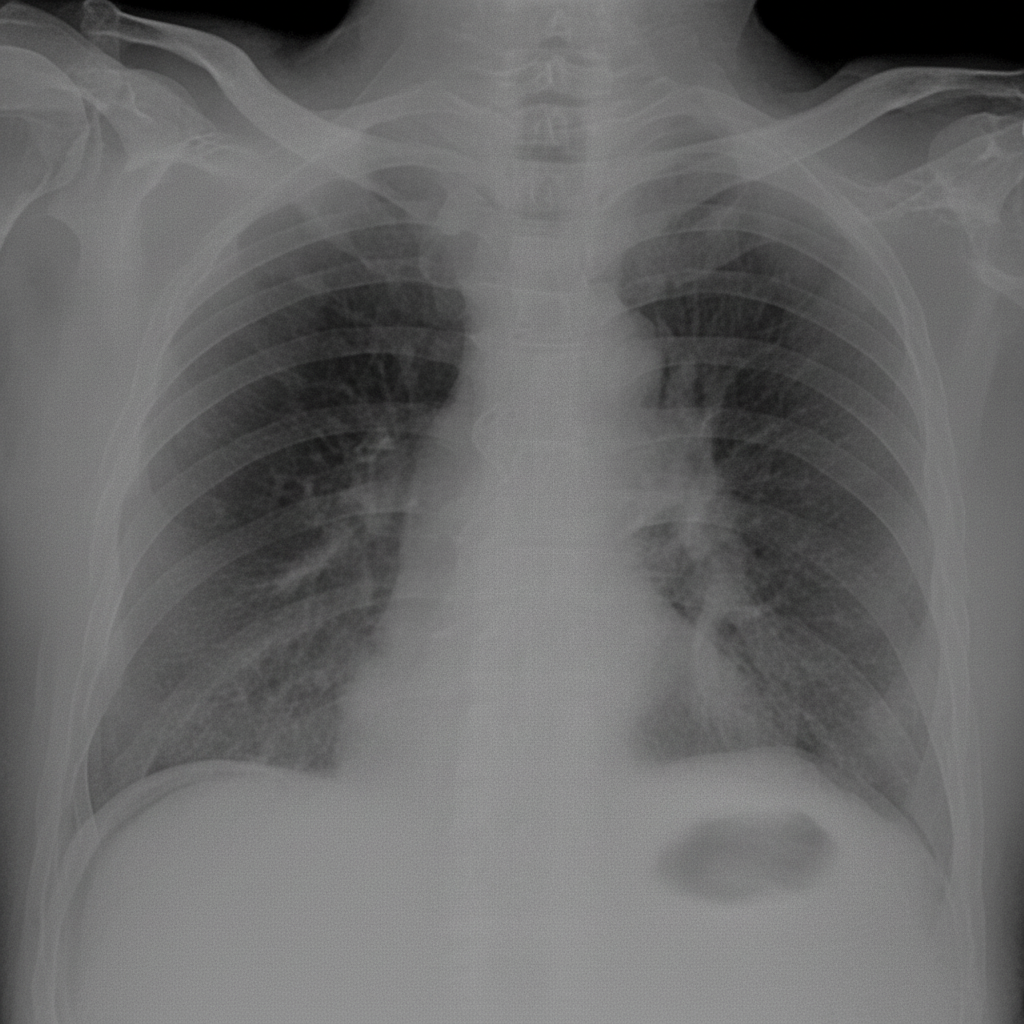
A plain radiograph of the chest and abdomen shows findings suggestive of which of the following conditions?
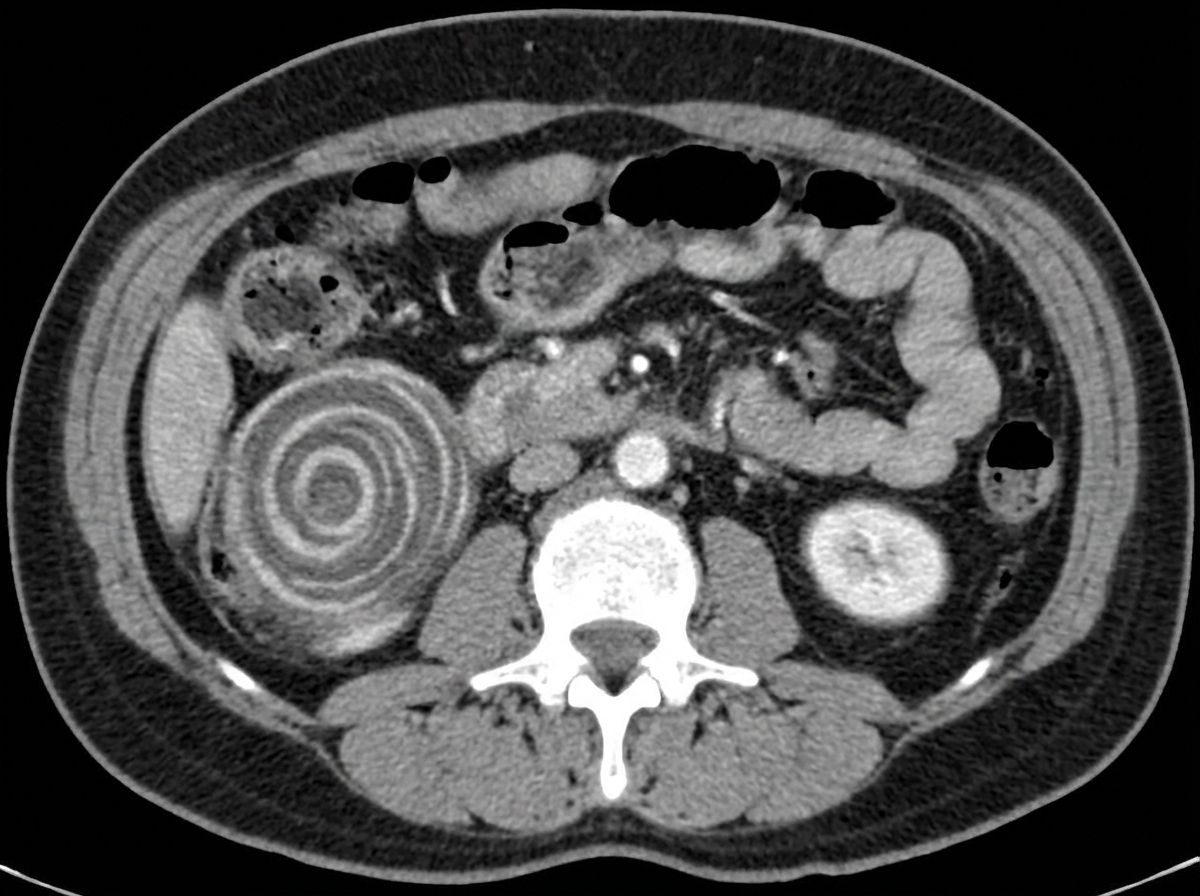
A 51-year-old male presents with blood-stained stools and abdominal pain. Based on the image shown, what is the most likely diagnosis?
'Rim' and 'ball' nephrograms in intravenous urography are seen in which condition?
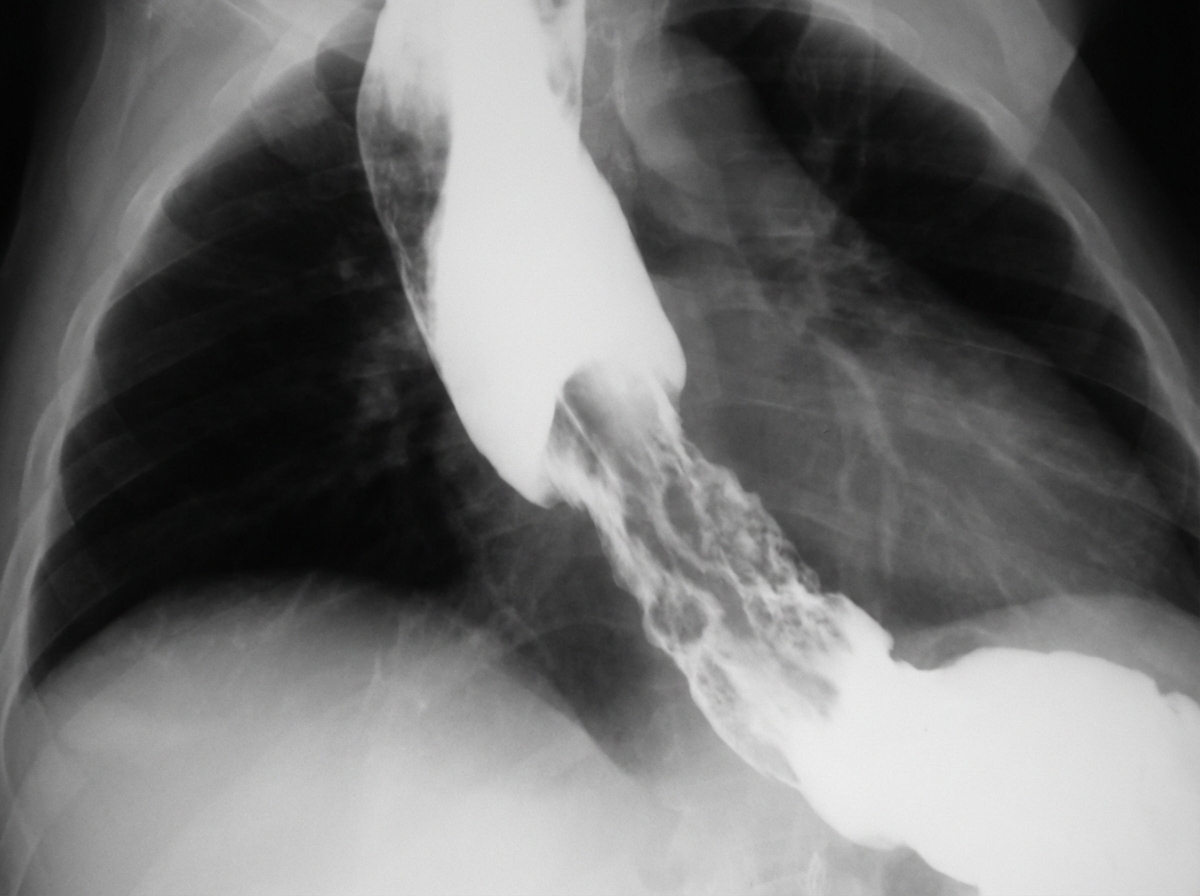
A 64-year-old man develops increasing dysphagia over many months. A barium swallow is performed. What is the most likely cause of his clinical presentation?
Tear-drop bladder is seen in which of the following conditions?
Which of the following is the most sensitive imaging modality for the diagnosis of idiopathic chronic pancreatitis (IOC)?
Which of the following is NOT a radiological feature of sigmoid volvulus?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app