
Abdominal and Pelvic Radiology — MCQs

On this page
A patient presents with right iliac fossa pain for 48 hours. USG image (shown with Doppler) demonstrates a hyperaemic appendix-region structure with surrounding inflammatory changes. There is no free fluid or evidence of perforation on USG. What is the most appropriate next step?
An elderly female patient presents to the emergency department with acute onset left flank pain radiating to the groin. What is the most appropriate imaging protocol for initial evaluation?
A 58-year-old male presents with a 3-month history of altered bowel habits, passage of blood mixed with stool, and a 6 kg weight loss. Colonoscopy was incomplete due to a tight stricture in the sigmoid colon. A barium enema is performed and the image is shown in Image 3. Which radiological sign is demonstrated, and with which pathology is it classically associated?

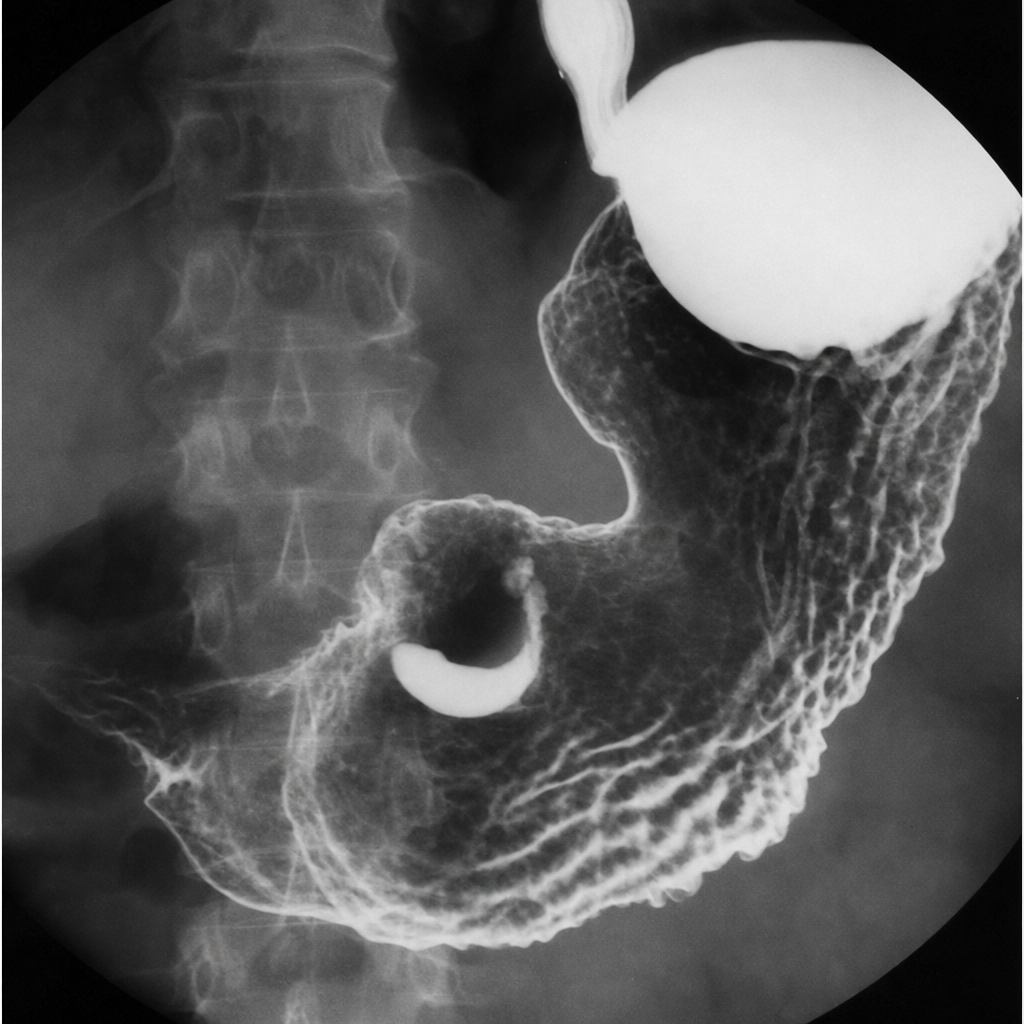
A 65-year-old male presents with a 4-month history of epigastric pain, early satiety, and progressive weight loss. He has a history of Helicobacter pylori infection treated 10 years ago. Haemoglobin is 9.2 g/dL. A barium meal fluoroscopy study is shown in Image 1. Which of the following best describes the radiological sign visible and its significance?
Which of the following radiographic presentations cannot be seen in a patient with intussusception?
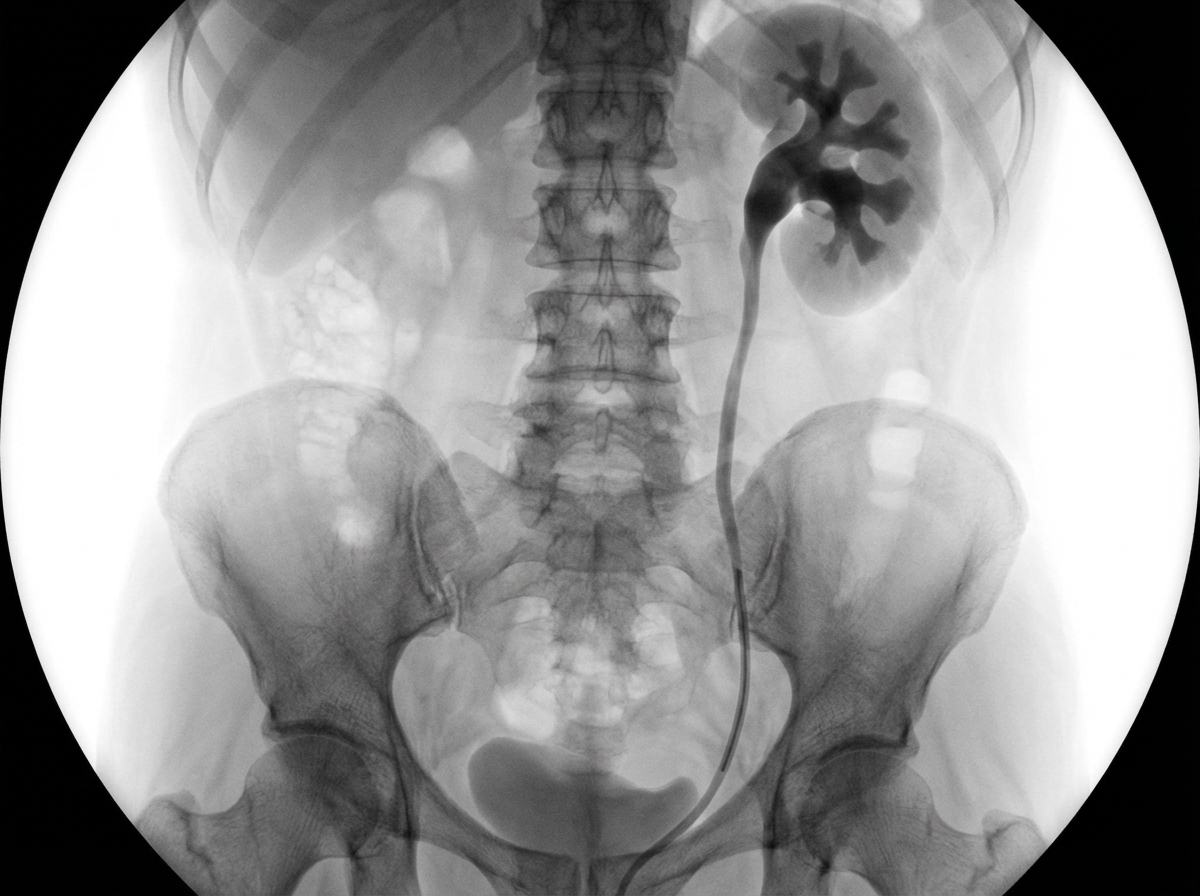
What is this study?
Which of the following conditions typically presents with a 'pseudokidney sign' on ultrasound?
Which of the following is NOT an ultrasound finding consistent with the diagnosis of adenomyosis?
Which condition is characterized by a 'doughnut' sign and 'coiled spring' appearance on imaging?
What is the typical CECT finding that suggests the diagnosis of pseudomyxoma peritonei?
Practice by Chapter
Imaging of Liver
Practice Questions
Biliary Tract Imaging
Practice Questions
Pancreatic Imaging
Practice Questions
Spleen and Lymphatic System
Practice Questions
Gastrointestinal Tract Imaging
Practice Questions
Renal and Urinary Tract Imaging
Practice Questions
Adrenal Imaging
Practice Questions
Female Pelvic Imaging
Practice Questions
Male Pelvic Imaging
Practice Questions
Abdominal Trauma Imaging
Practice Questions
Acute Abdomen Imaging
Practice Questions
Imaging of Peritoneal Cavity and Retroperitoneum
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app