
Psychotic Disorders — MCQs

On this page
General Paresis of the Insane is associated with which condition?
All of the following are features of hallucination EXCEPT:
Loss of insight is seen in which of the following conditions?
Somatic passivity is a feature of which of the following conditions?
A patient with schizophrenia is on neuroleptics. Their psychotic symptoms have improved, but they have developed sadness, talk less, and remain in bed. Which of the following is LEAST likely to be the cause of these new symptoms?
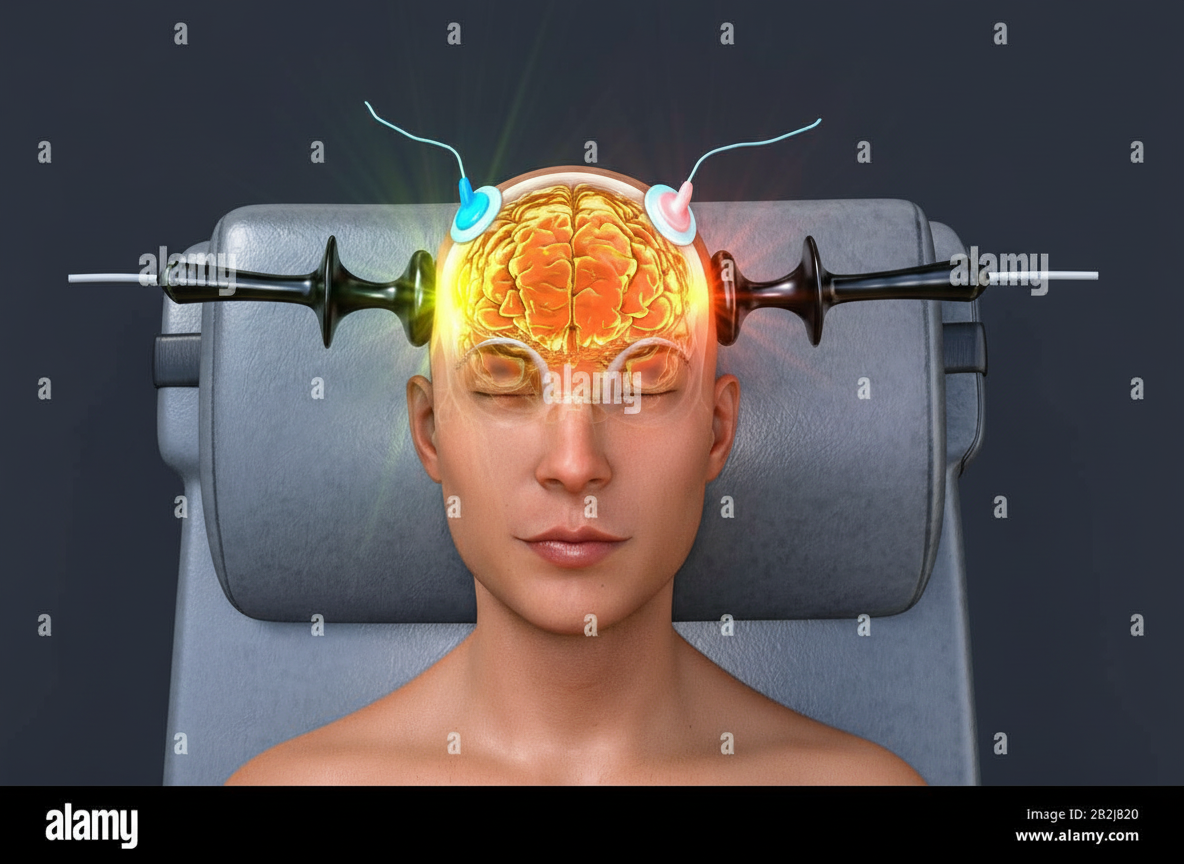
The procedure shown below is used in all of the following illnesses except:
Bleuler's symptoms of schizophrenia include which of the following?
Worst prognosis is seen in which type of schizophrenia?
A 33-year-old male traveling by flight started fighting with an air hostess. The man alleged that the air hostess was his wife, but she had changed her face so she could not be identified. This history is consistent with which of the following syndromes?
A 45-year-old male admits himself to the hospital, stating that the nurse treating him is an imposter, and his wife has replaced her to kill him. What is the most likely diagnosis?
Practice by Chapter
Schizophrenia: Epidemiology and Etiology
Practice Questions
Schizophrenia: Clinical Features
Practice Questions
Schizophrenia: Treatment
Practice Questions
Schizoaffective Disorder
Practice Questions
Delusional Disorders
Practice Questions
Brief Psychotic Disorder
Practice Questions
Substance-Induced Psychotic Disorders
Practice Questions
Psychosis in Medical Conditions
Practice Questions
First Episode Psychosis
Practice Questions
Treatment-Resistant Psychosis
Practice Questions
Rehabilitation in Psychotic Disorders
Practice Questions
Outcome and Prognosis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app