
Cardiovascular System — MCQs

On this page
A 75-year-old woman is admitted to the hospital with anginal pain. The ECG reveals myocardial infarction and a right bundle branch block. During physical examination, the patient has a loud second heart sound. Which of the following heart valves are responsible for the production of the second heart sound?
QT shortening is associated with which electrolyte imbalance?
The organ with maximum blood flow in milliliters per kilogram per minute during resting is:
In the context of hypoxia, the cardiovascular response to peripheral chemoreceptor stimulation can result in which of the following changes in heart rate?
Hypotension in acute spinal injury is due to:
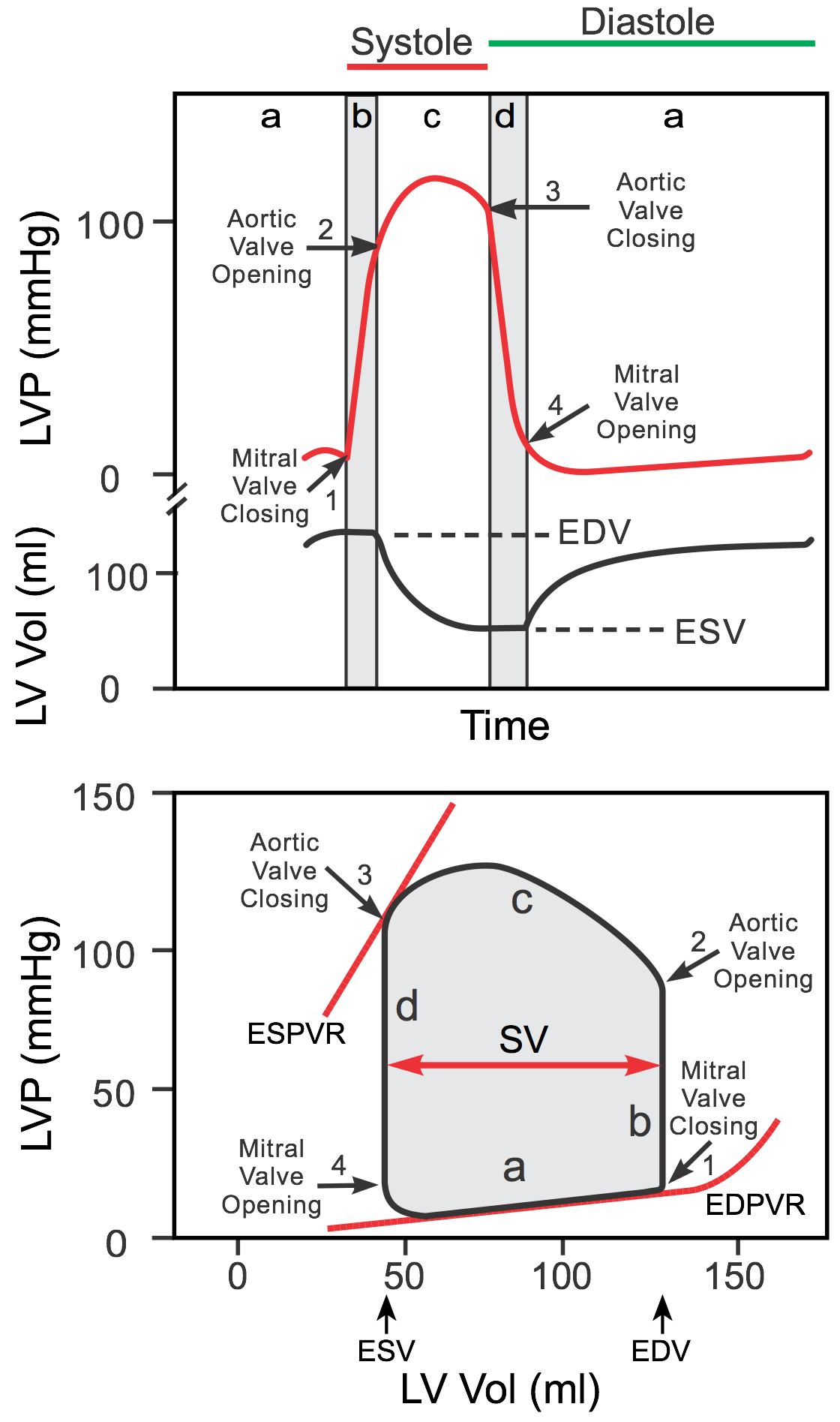
Pressure-Volume loop of cardiac cycle is shown below. What does point C represent?
The primary effect of vagal stimulation on the heart is
A shift of posture from supine to upright posture is associated with cardiovascular adjustments. Which of the following is NOT true in this context?
What is the mean arterial pressure (MAP) for a person with an arterial blood pressure of 125/75 mm Hg?
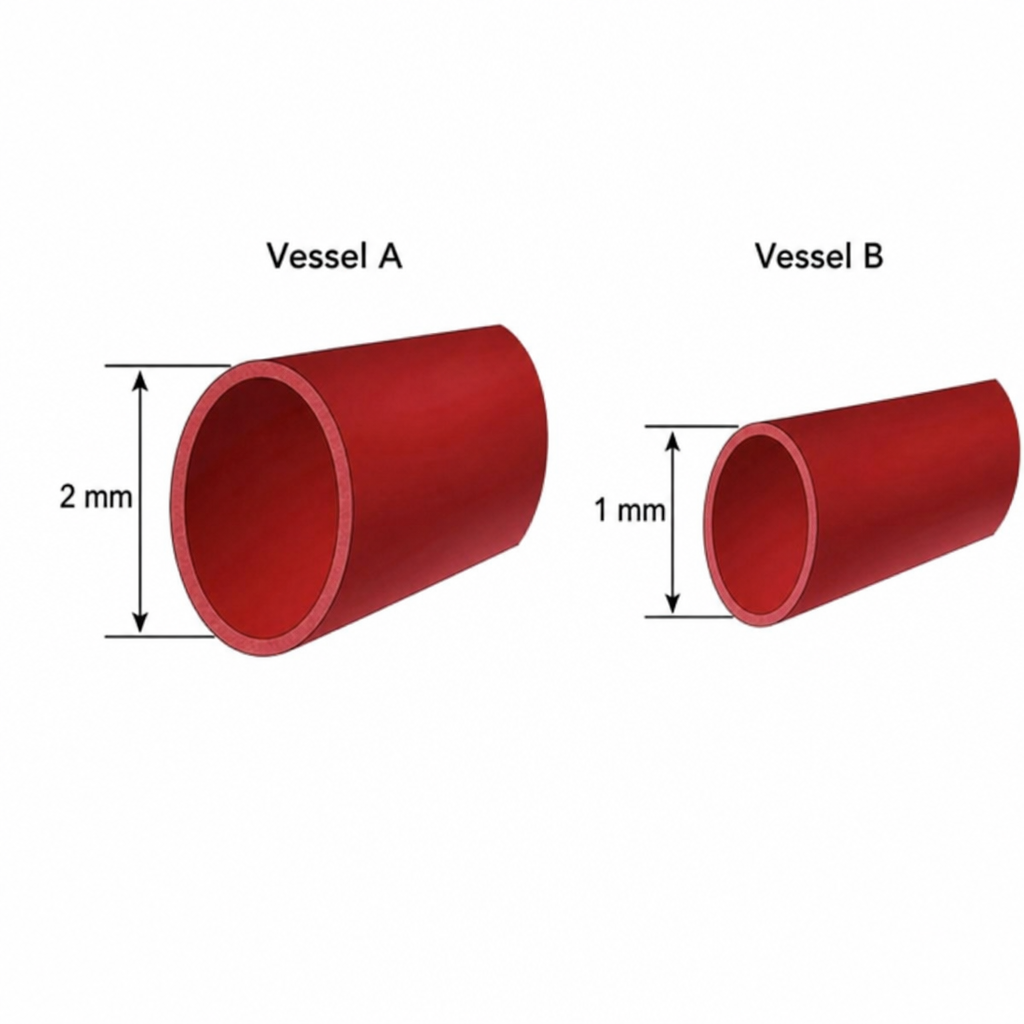
Below are two vessels shown. Assuming both vessels have equal lengths, equal pressure gradients, and the same blood viscosity, and both of them follow linear flow pattern, what will be the amount of blood flow in vessel A compared to vessel B?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app