
Cardiovascular System — MCQs

On this page
Gas exchange in tissues takes place at?
What does Einthoven's law state regarding the relationship between the electrical potentials of the limb leads?
Mechanism by which Ach decreases heart rate is by:
Which of the following factors increases stroke volume?
What is the normal range of interstitial pressure?
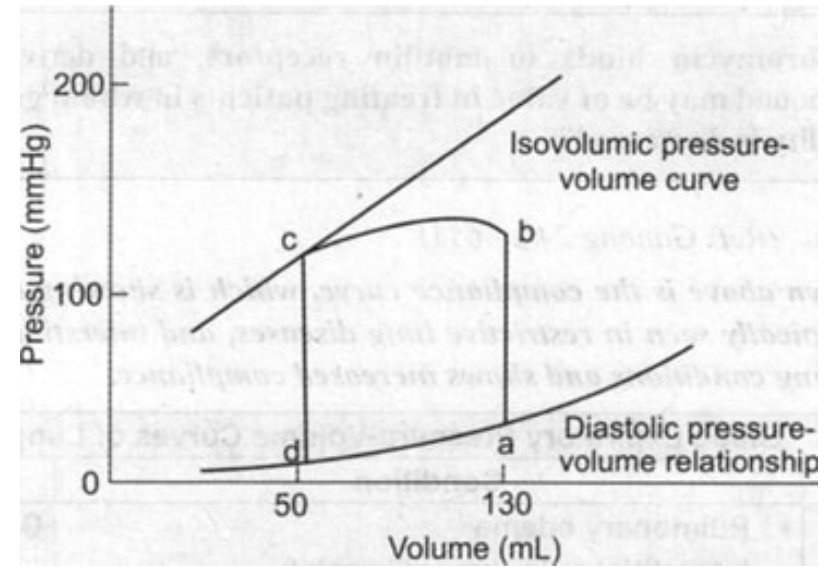
From the given pressure-volume curve, identify the end-diastolic volume (EDV) and end-systolic volume (ESV), then calculate the ejection fraction using the formula EF = (EDV - ESV)/EDV × 100%.
Which of the following statements about volume receptors is NOT true?
Which one of the following is the CORRECT statement regarding coronary blood flow?
Which of the following components are included in microcirculation?
What is the definition of preload in the context of cardiac physiology?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app