
Cardiovascular System — MCQs

On this page
What is the equilibrium pressure in the absence of flow called?
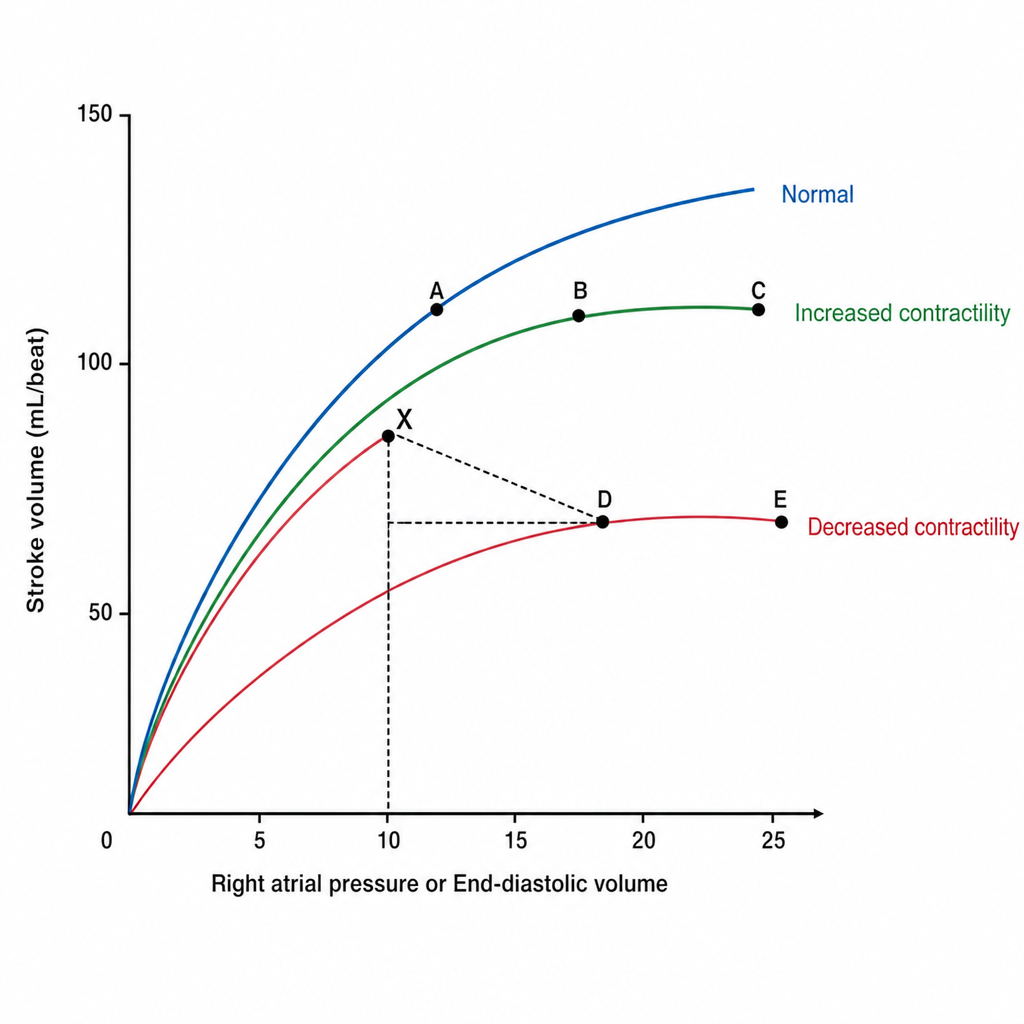
An increase in afterload and venous compliance can cause stroke volume to change from the point marked X to which point?
In a standard Electrocardiogram, an augmented limb lead measures the electrical potential difference between which points?
Acetylcholine decreases heart rate by:
Which of the following is the last part of the ventricle to be depolarized?
Increase in heart rate just before starting exercise is due to?
Massage of the carotid sinus results in all of the following, EXCEPT:
A 60-year-old patient with a 25-year history of hypertension underwent renal artery Doppler, which showed narrowing and turbulence in the right renal artery. If the diameter of the lumen is reduced by 50%, by how much will the blood flow be reduced?
Peripheral resistance is maximum in which of the following?
A patient has an aerial blood pressure of 90 mm Hg and a cardiac output of 5.4 L/min. What is the peripheral resistance?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app