
Cardiovascular System — MCQs

On this page
All of the following peptides produce vasodilation in most vascular beds EXCEPT?
Which amongst the following endothelin is involved in myocardial infarction?
What is the cardiac cycle duration in seconds for a person with a heart rate of 75 beats per minute?
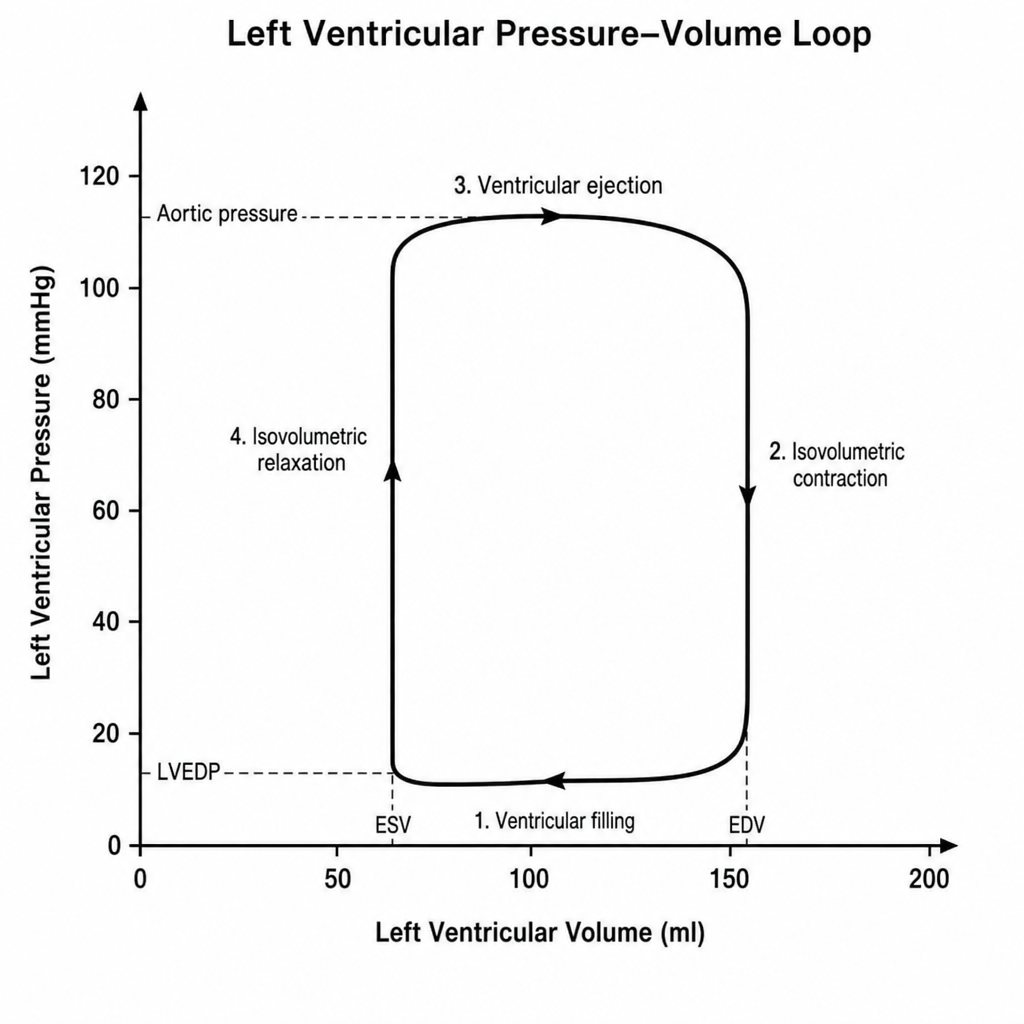
A left ventricular pressure-volume loop is shown. During exercise within physiological limits, what is the effect on end-systolic volume?
What is the action of Atrial Natriuretic Peptide (ANP)?
How does chronic hypertension affect the range of arterial pressure over which the cerebral circulation can maintain relatively constant blood flow?
Which statement is true regarding heart sounds?
Blood flow in the splanchnic area during exercise is decreased due to which of the following mechanisms?
The following ECG findings are seen in hypokalemia:
Cardiac muscle is able to function as a syncytium because of the structural presence of which of the following?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app