
Cardiovascular System — MCQs

On this page
All of the following increase blood pressure except:
Which part of the action potential in cardiac pacemaker cells is primarily affected by calcium channel blockers?
Which of the following neurotransmitters is primarily released from the sympathetic nervous system to increase heart rate in response to a DECREASE in blood pressure?
Which of the following statements about cardiac muscle is incorrect?
Which phases occur in the sequence: rapid filling followed by atrial contraction?
What is the correct sequence of phases that follows isovolumic contraction in the cardiac cycle?
How does pulmonary hypertension contribute to hemoptysis?
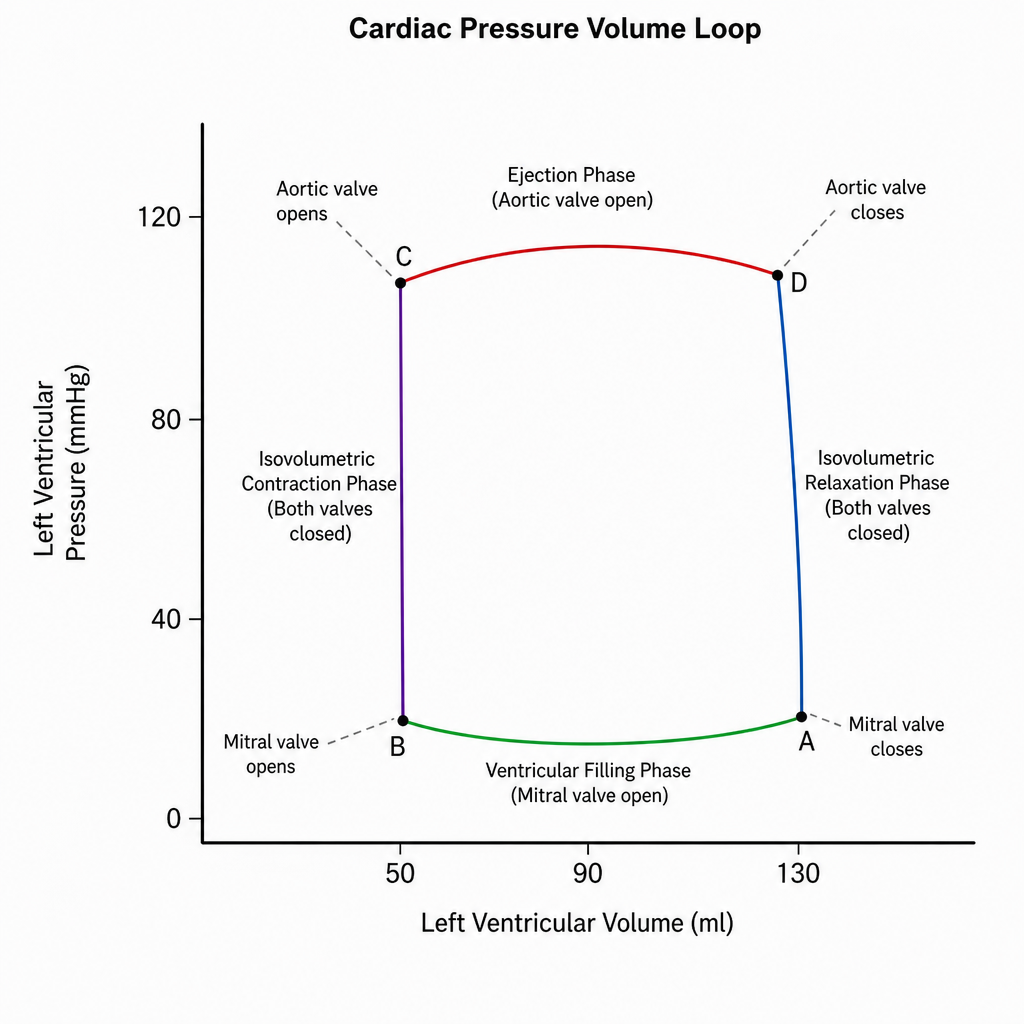
During the cardiac cycle, which phase corresponds to the period when the ventricles are contracting but no blood is being ejected?
The Bainbridge reflex is triggered by:
In the cardiac pressure-volume loop, which phase corresponds to isovolumetric contraction?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app