
Cardiovascular System — MCQs

On this page
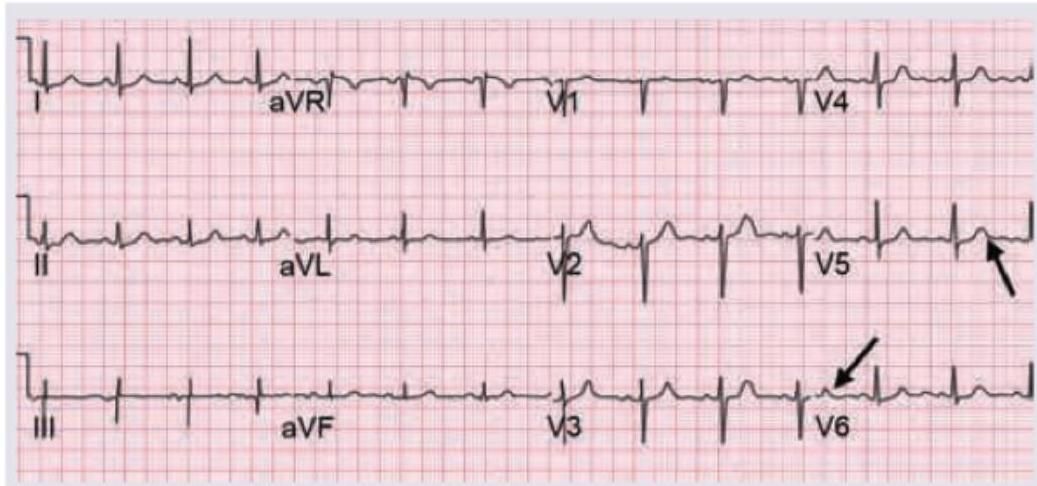
The normal amplitude of the marked wave is usually less than \qquad mm in the chest leads.
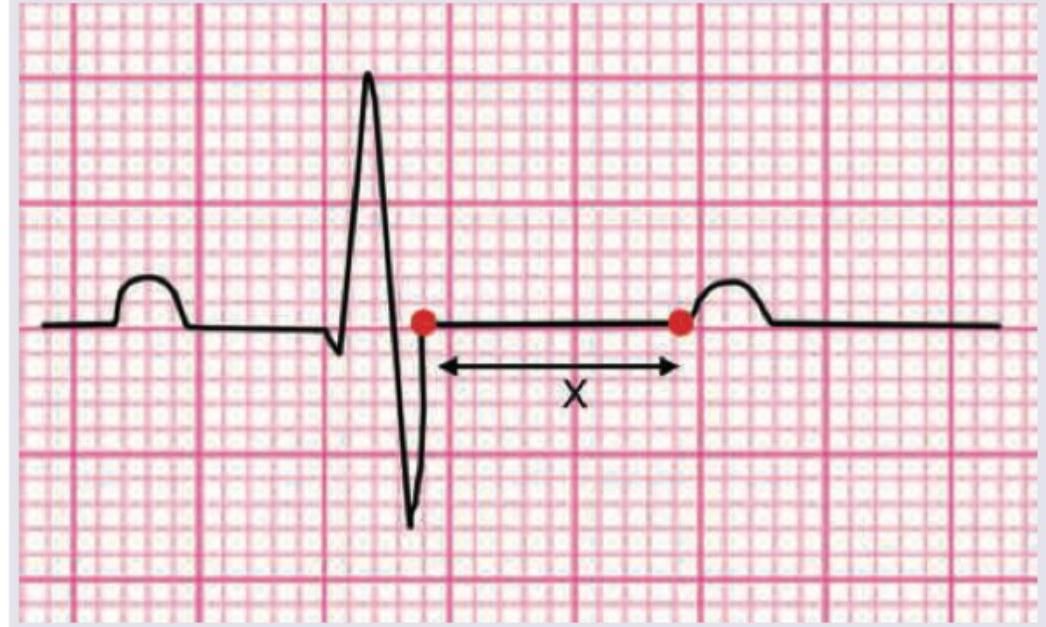
The marked part of the ECG called as 'X' points to which phase of cardiac action potential?
Distributive shock is described by which of the following patterns of cardiovascular responses? 1. Vasodilation 2. Reduced peripheral vascular resistance 3. Inadequate 'afterload' 4. Low cardiac output Select the correct answer using the code given below.
Which one of the following statements is not correct about fetal circulation?
Non-cardiac causes of raised central venous pressure include all of the following except:
The central venous pressure (CVP) is low in
What is the function of the umbilical artery in fetal circulation?
Which among the following organs has the least arteriovenous oxygen difference?
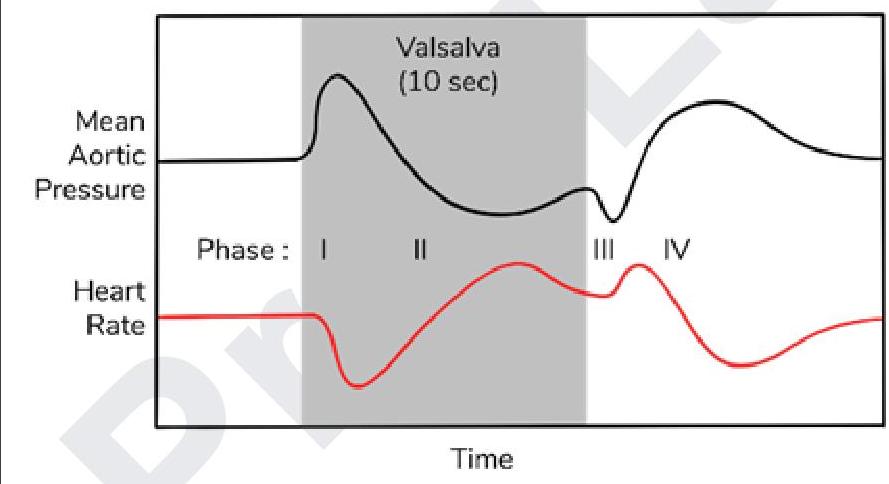
Blood pressure changes in radial artery were measured. Which of the following is the reason for initial rise in BP while performing Valsalva maneuver?
Windkessel effect is not shown by which of the following vessel?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app