
Cardiovascular System — MCQs

On this page
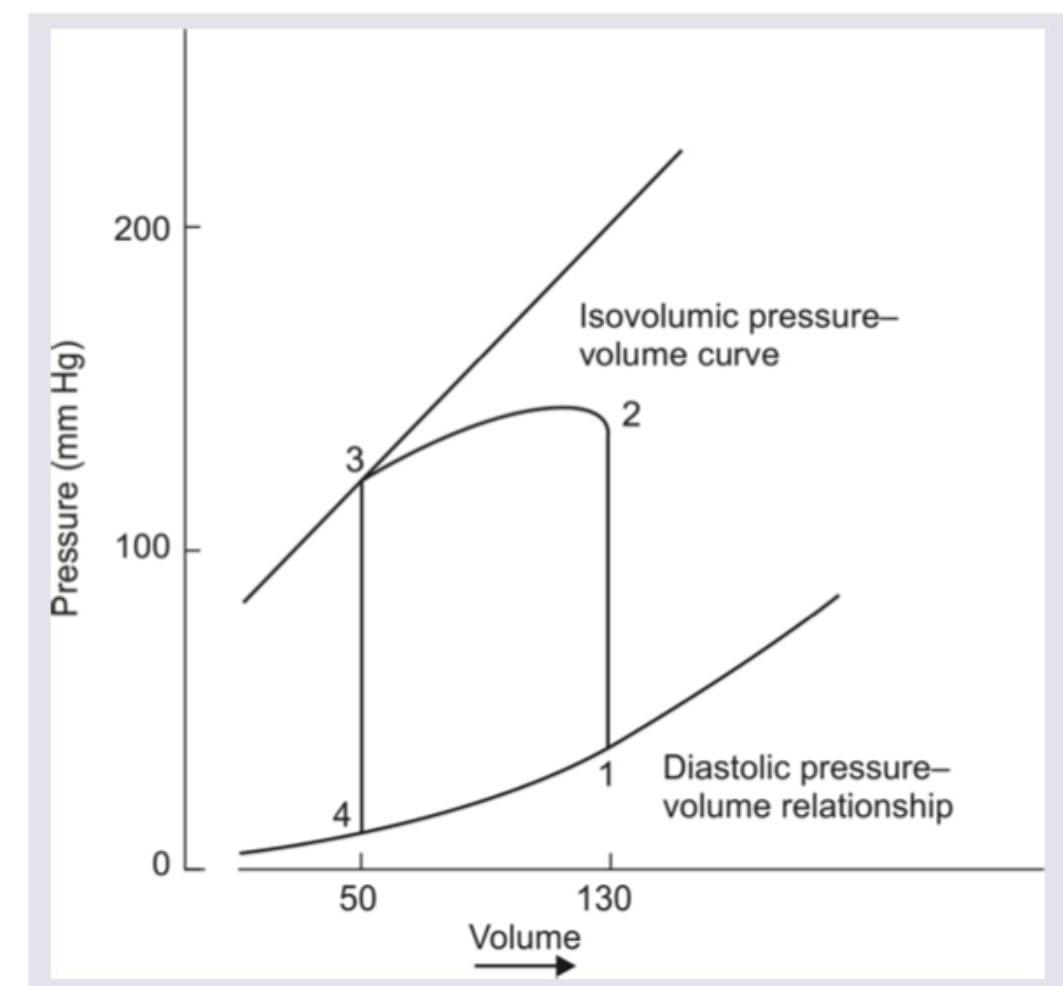
Which of the following is correct about the pressure volume loop of left ventricle?
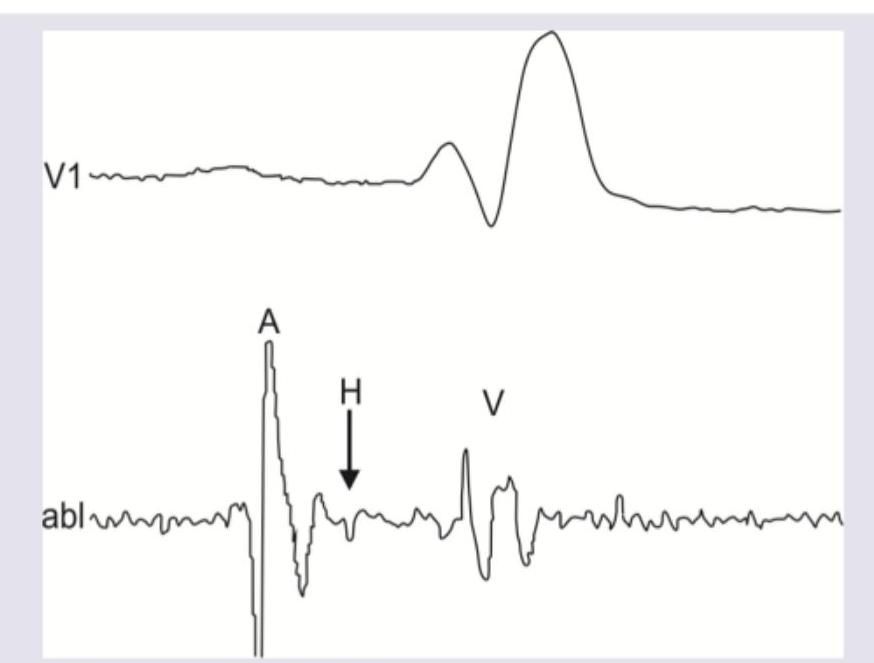
The A wave in His bundle electrogram shows presence of:
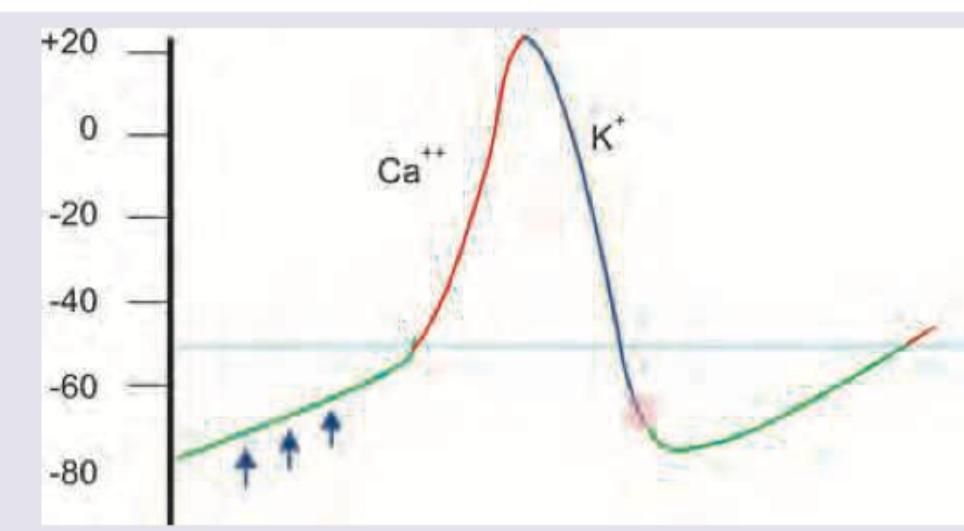
The phase of cardiac action potential marked Green is predominantly initiated by which of the following currents?
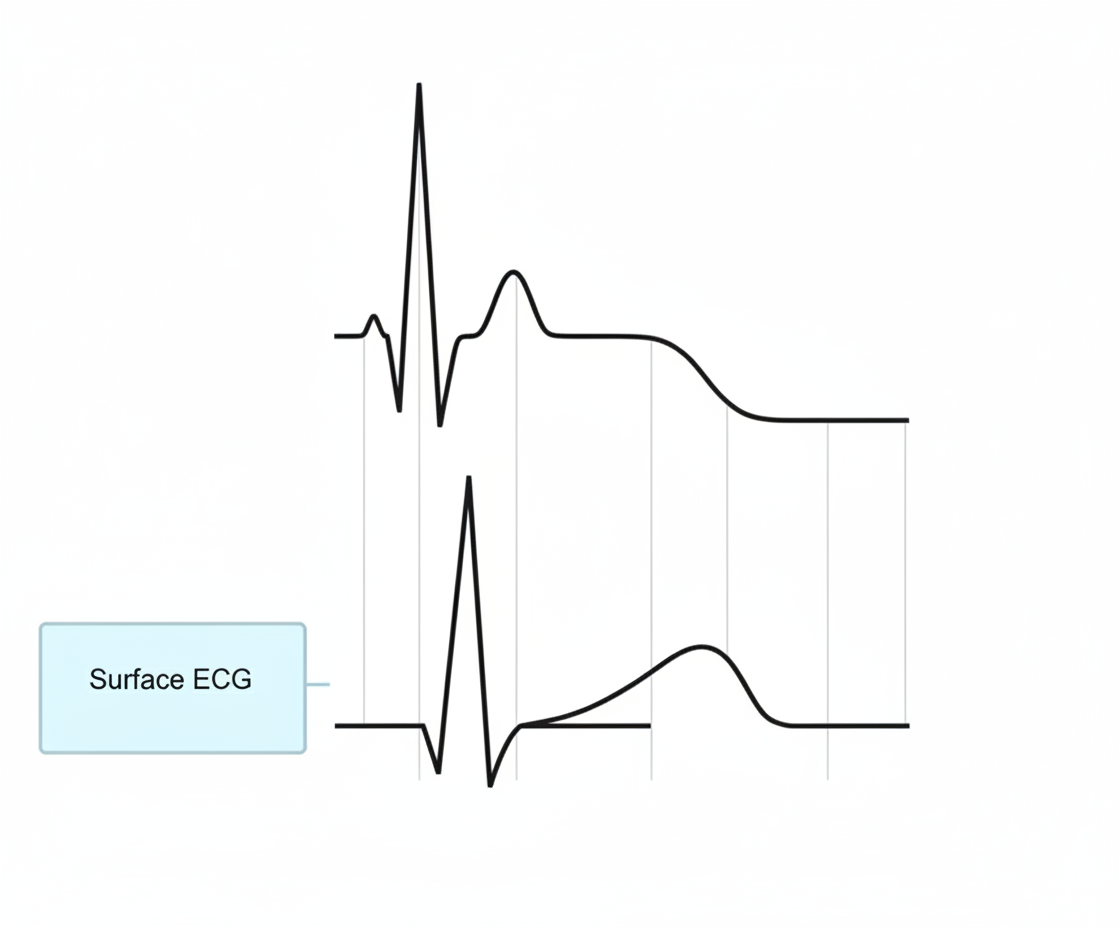
Which part of ventricular action potential corresponds to ST segment in ECG?
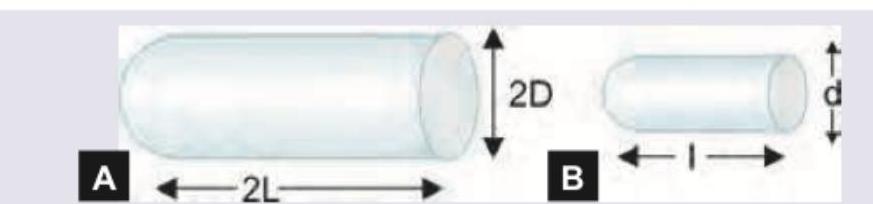
There are two blood vessels shown below. Both vessels carry the same fluid (equal viscosity) under the same pressure difference, and both follow steady laminar flow. Vessel A has diameter 2d and length 2L; vessel B has diameter d and length L. What will be the amount of blood flow in A compared to B?
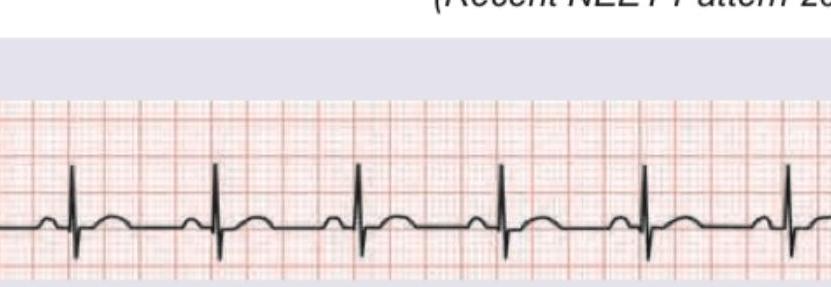
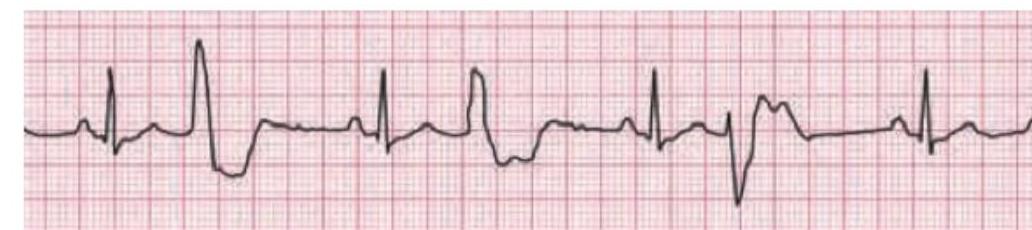
Compare the two ECG recordings taken before and after activation of low pressure atrial stretch receptors. Which reflex explains the findings?
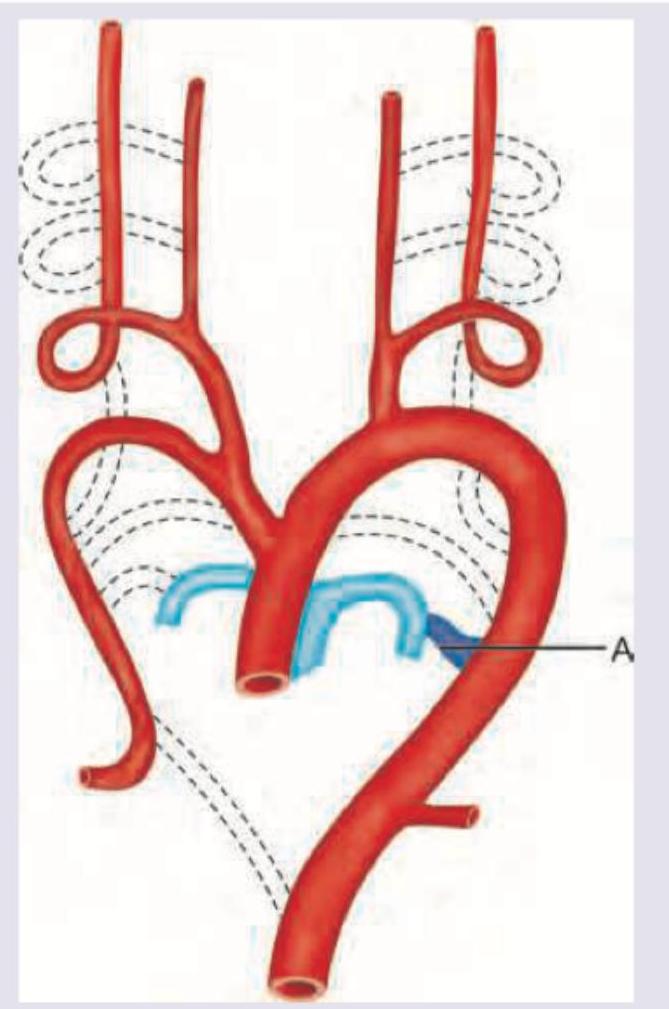
The structure marked $A$ begins to close by what time frame and due to what cause?
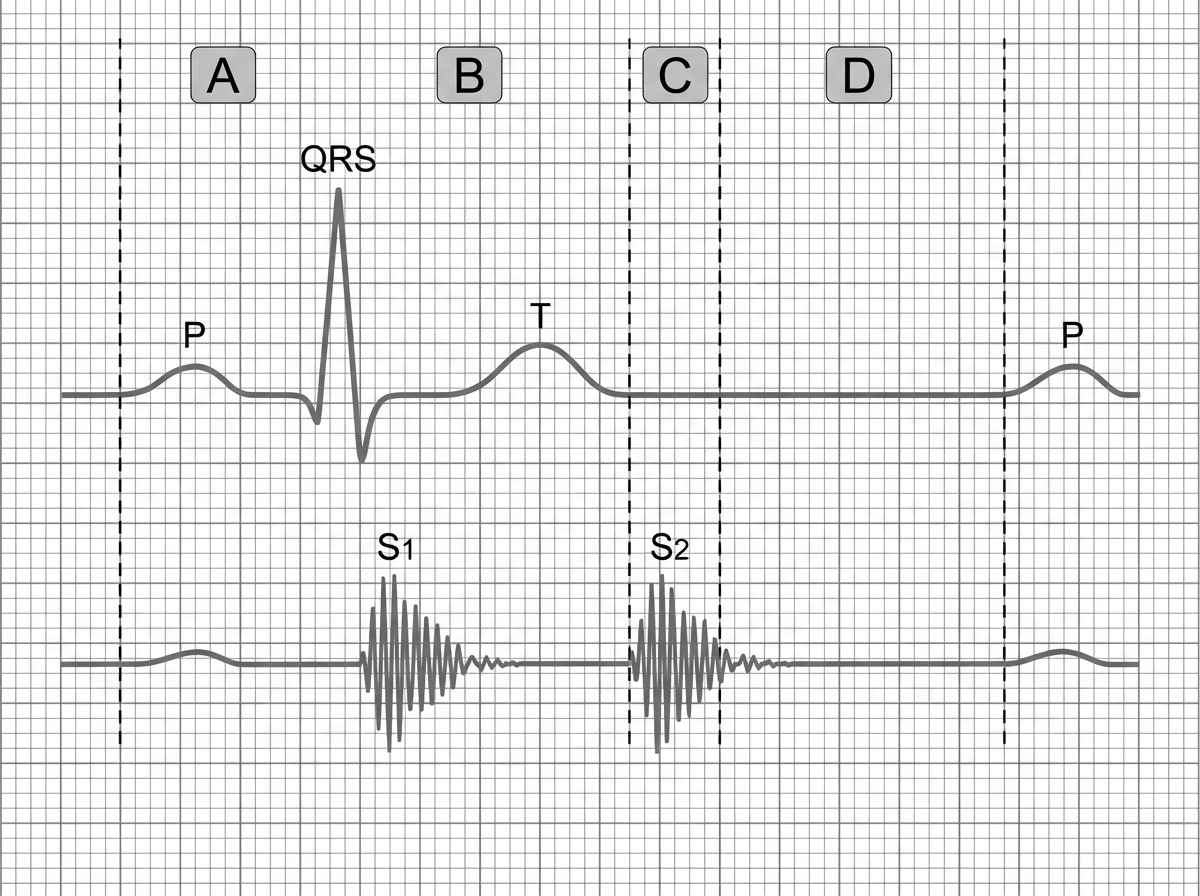
Phonocardiogram tracing is shown below with corresponding ECG. Identify the phase corresponding with $S_{2}$ in phonocardiogram.
Using the quadrant method, if the mean QRS vector in lead I is negative and in lead aVF is positive, what is the axis?
If the mean QRS vector in lead I is positive, in lead II is negative, and in lead III is negative, what is the axis deviation?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app