
Cardiovascular System — MCQs

On this page
A patient presents with high blood pressure accompanied by a decrease in heart rate. What is the most likely physiological mechanism responsible for this response?
Scientists administered norepinephrine to guinea pigs, resulting in an increase in systolic and diastolic blood pressure and a decrease in heart rate. What mechanism explains this response?
The first heart sound coincides with which cardiac cycle phase?
Which of the following are features of Bezold Jarisch reflex? 1. Bradycardia 2. Hypertension 3. Coronary vasodilation 4. Tachycardia
Which type of pulse is based on the Frank-Starling law?
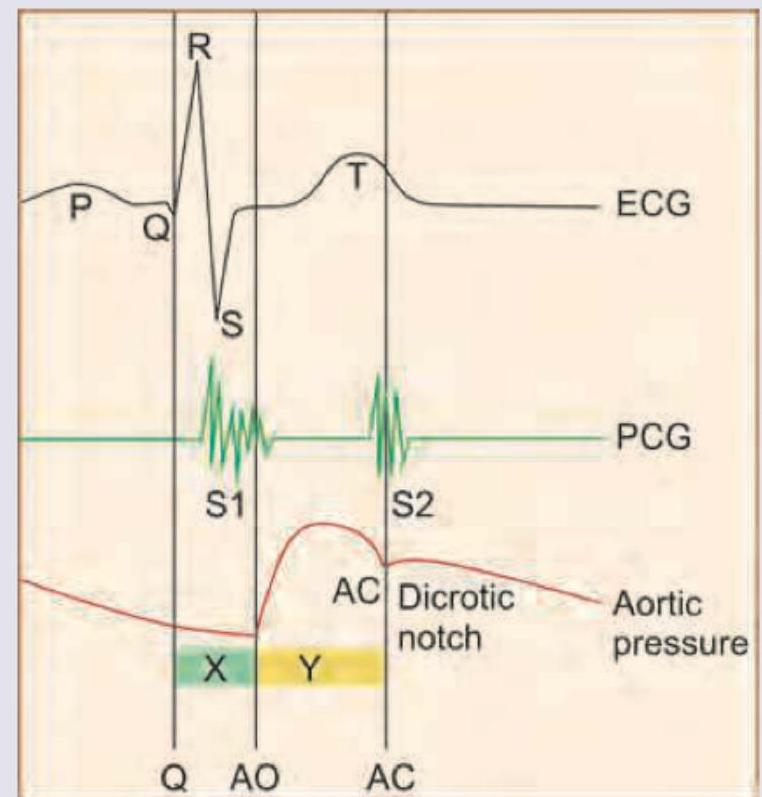
The recording of cardiac cycle is drawn below. Which of the following is correct about $X$ and $Y$ shown in the image?
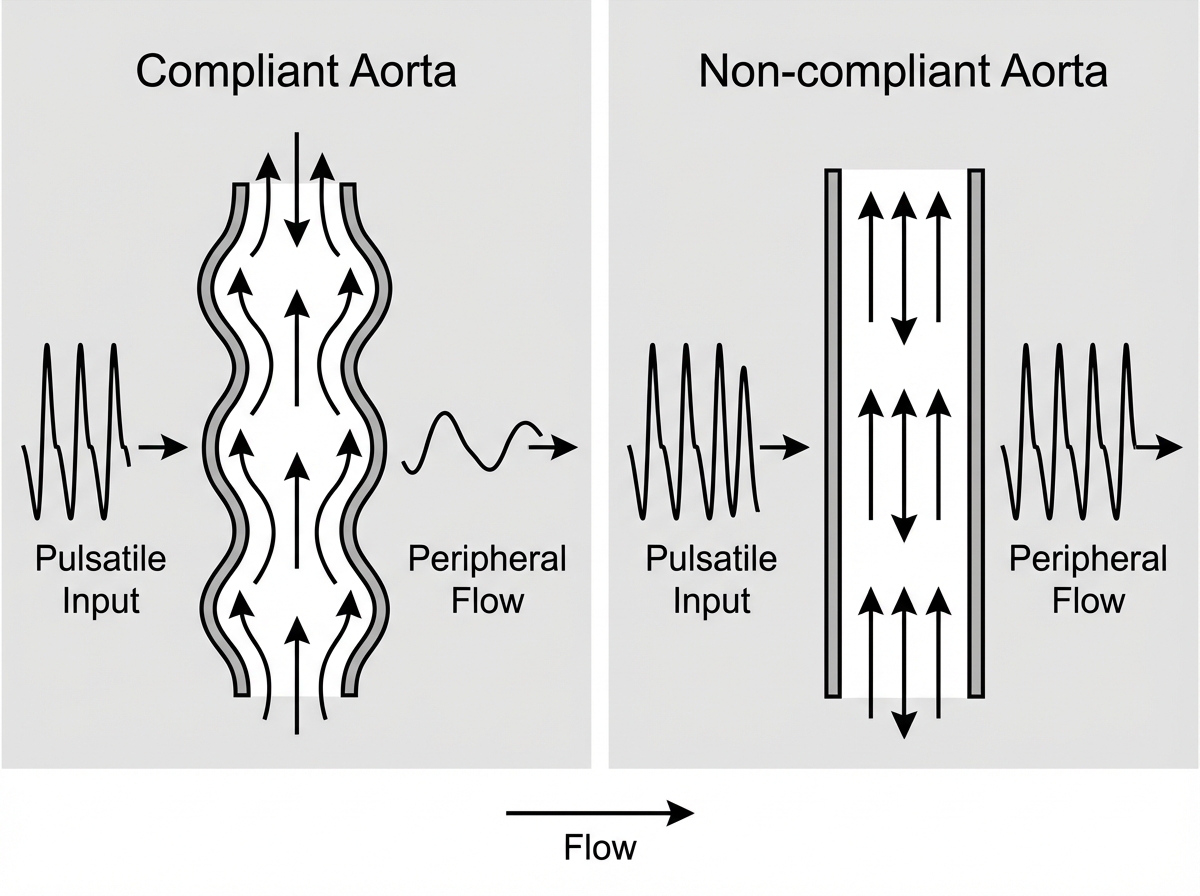
The following diagram represents flow in compliant versus non-compliant aorta. This shows operation of:
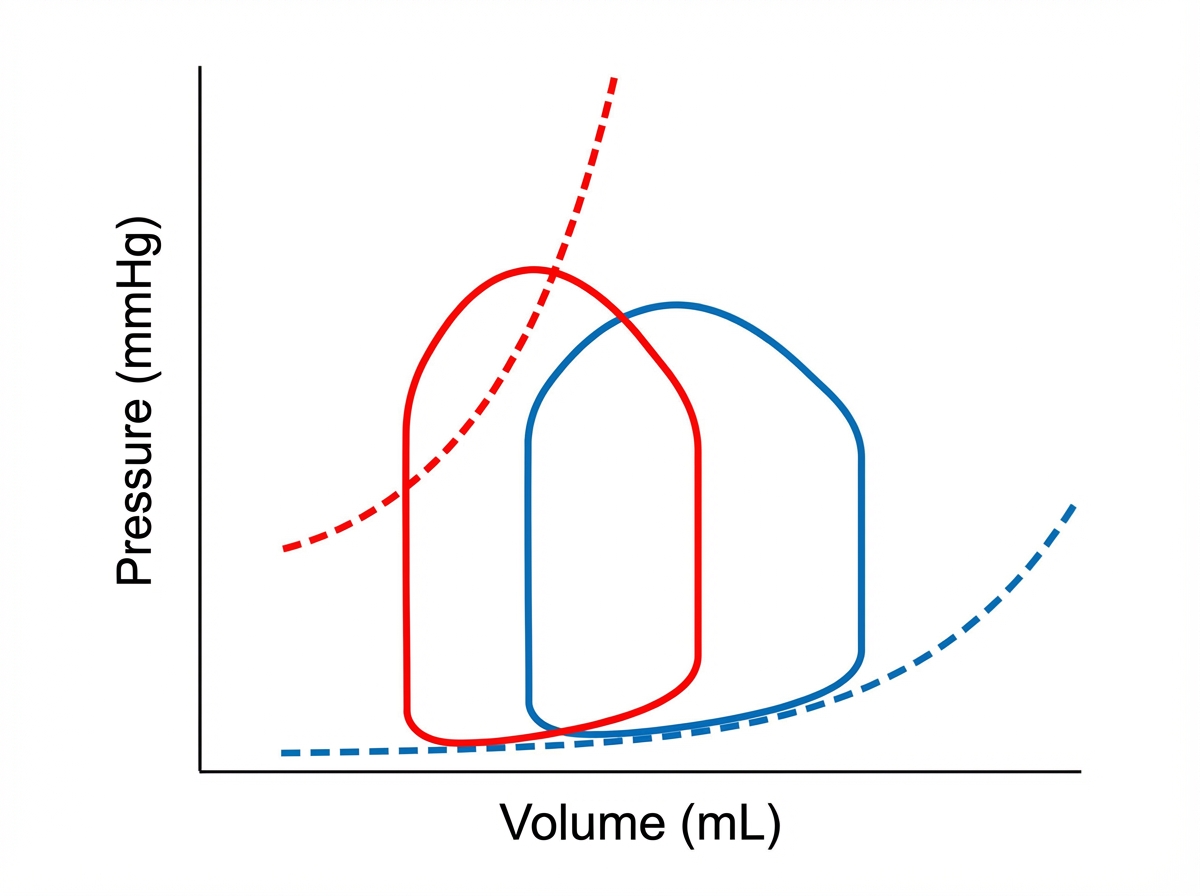
The pressure-volume loop of left ventricle tracing of the patient indicates:
Which of the following is correct about the point marked $Z$ on the cardiac cycle?
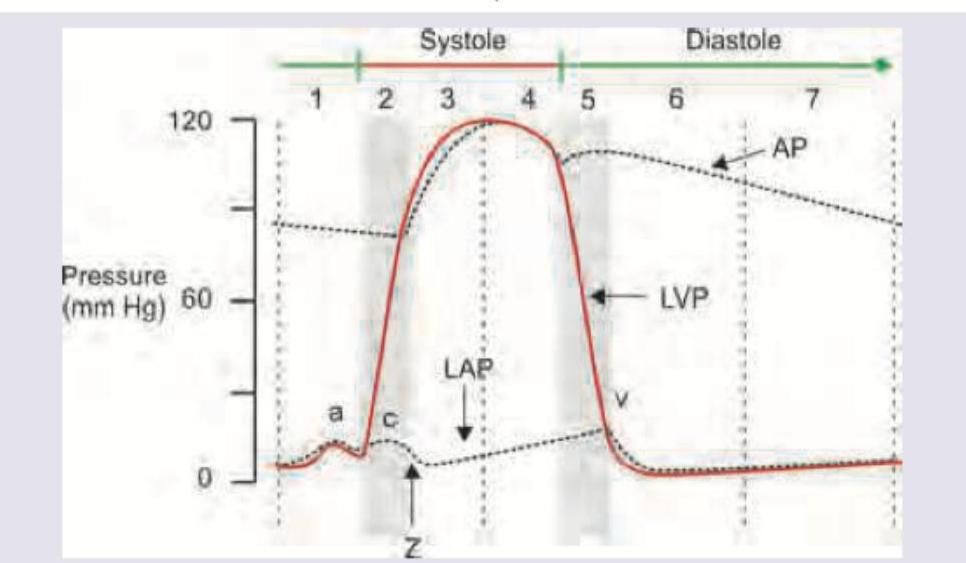
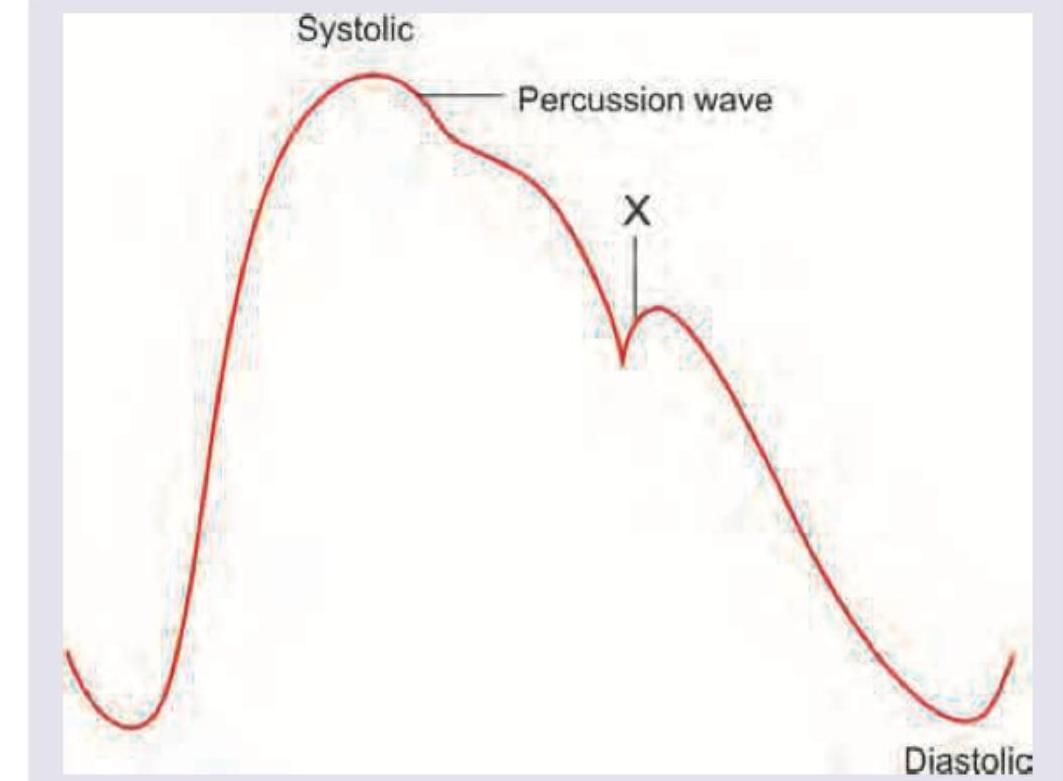
Which of the following is correct about the 'X' marking in Arterial Waveform?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app