
Cardiovascular System — MCQs

On this page
Cardiac output is increased by all except?
The depressor reflex, also known as the Bezold-Jarisch reflex, is produced by which of the following stimuli?
Maintenance of blood pressure according to intracranial pressure is described by which reflex?
A 60-year-old patient underwent renal artery Doppler which shows narrowing and turbulence in the right renal artery. If the radius of the artery is reduced by 1/3rd, by how many times would resistance to blood flow in the right kidney have increased?
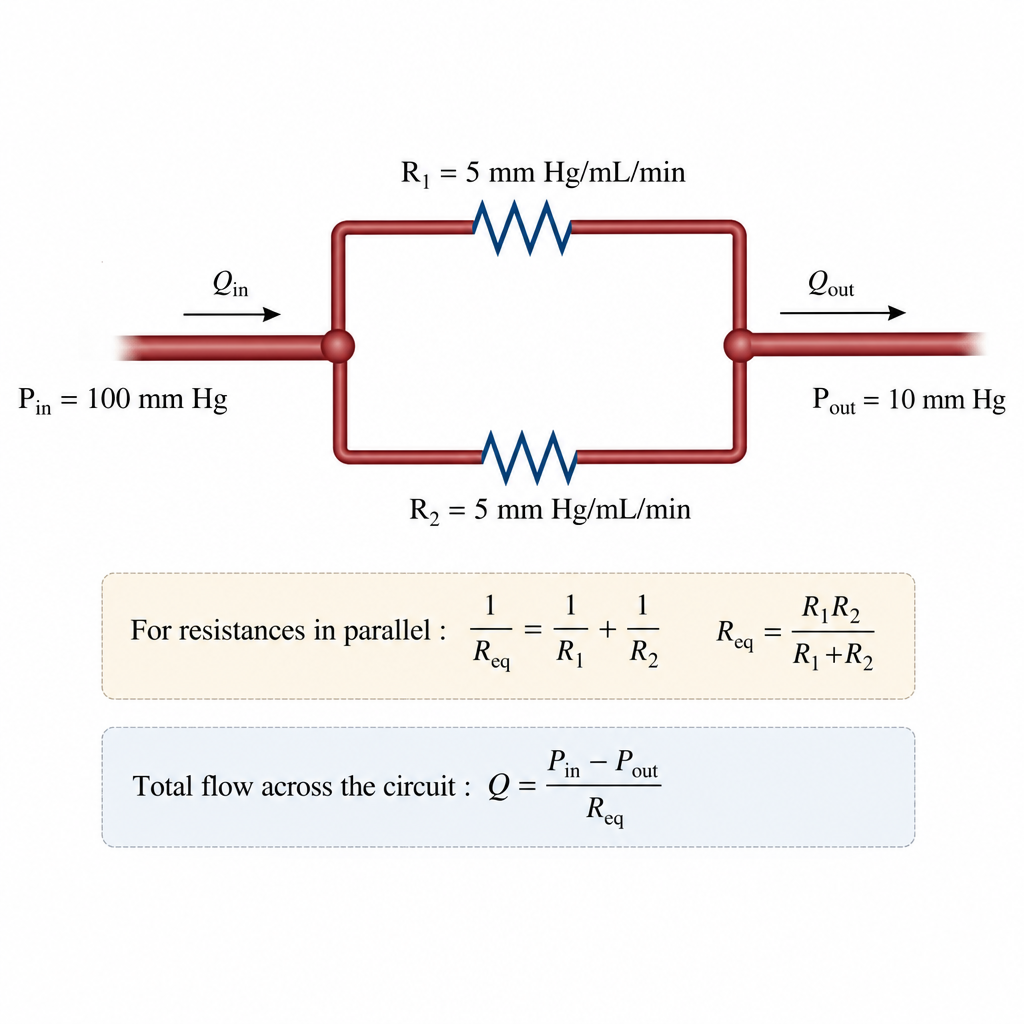
In a parallel circuit, the inflow pressure is 100 mm Hg and the outflow pressure is 10 mm Hg. Each of the parallel circuit has a resistance of 5 mm Hg/mL/min. Calculate the flow across the circuit.
Which organ has the most permeable capillaries?
In a parallel circuit, the inflow pressure is 100 mm Hg and the outflow pressure is 10 mm Hg. Each of the parallel circuit has a resistance of 5 mm Hg/mL/min. Calculate the flow across the circuit.
Which substance is NOT synthesized by the vascular epithelium?
Which of the following is a feature of shock?
In the jugular venous pressure (JVP) waveform, the "a" wave corresponds to:
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app