
Cardiovascular System — MCQs

On this page
A 43-year-old woman is diagnosed with mitral valve stenosis. During physical examination, the first heart sound is abnormally loud. Which of the following heart valves are responsible for the production of the first heart sound?
In the presence of a drug that blocks all effects of norepinephrine and epinephrine on the heart, the autonomic nervous system can:
Veins are an example of which type of blood vessel?
Which of the following statements about healthy, intact capillaries is true?
A decrease in cerebral blood flow to zero causes death of brain tissue within what timeframe?
What physiological event occurs during isovolumetric contraction?
The 'a' wave is absent in which of the following conditions?
Orthopnea in heart failure develops due to which of the following?
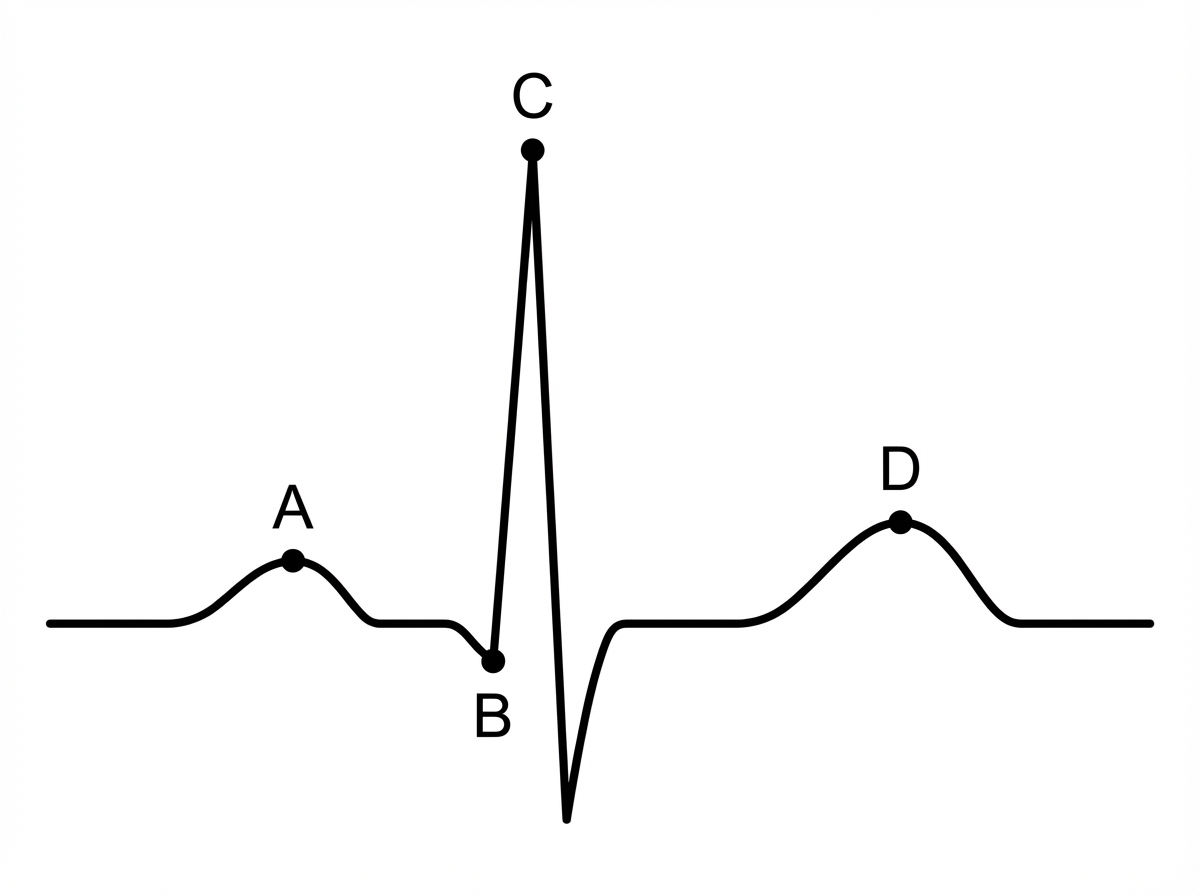
In the diagram below, which labeled point represents the "R" wave of ventricular depolarization?
What is the characteristic ECG change observed in hyperkalemia?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app