
Cardiovascular System — MCQs

On this page
An ECG obtained from a 57-year-old male during a routine physical examination reveals atrial fibrillation. Which is most likely to accompany this condition?
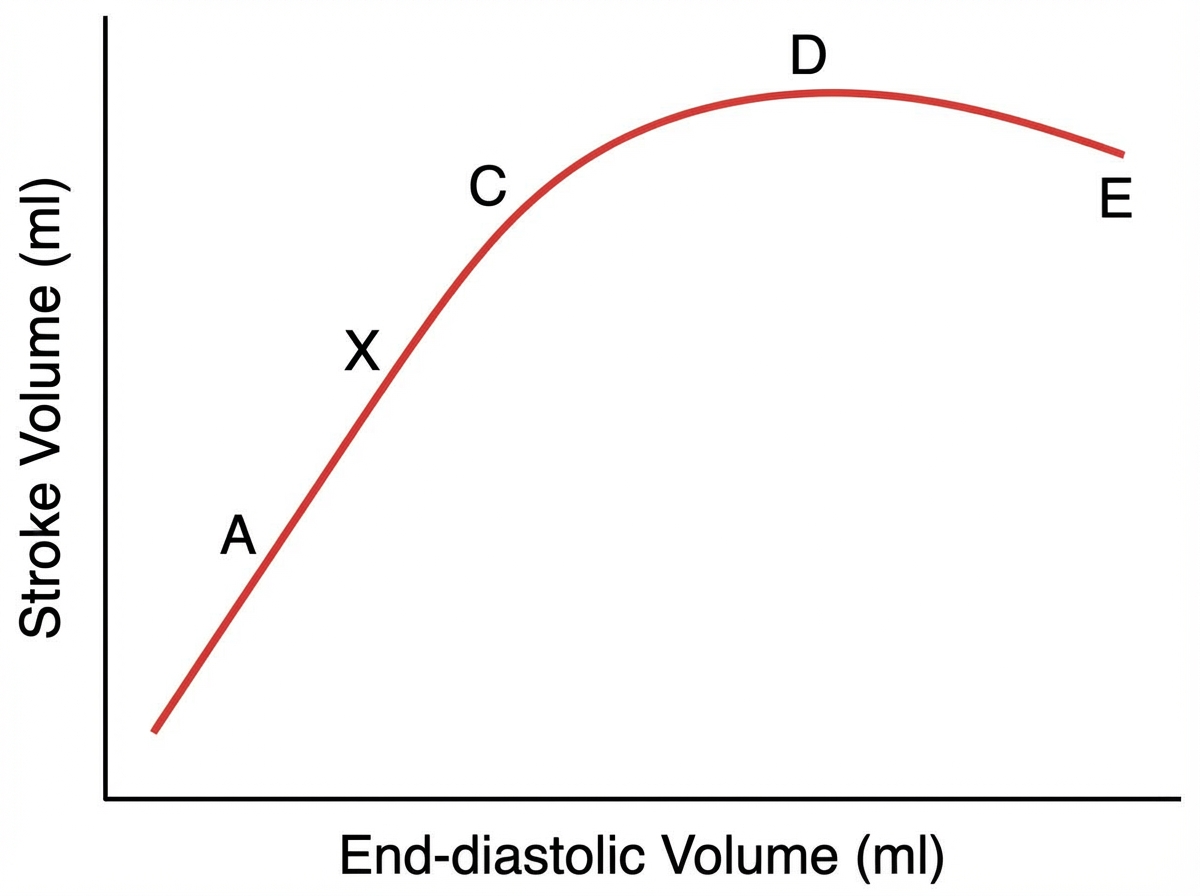
A mild hemorrhage will cause stroke volume to shift from point X to which of the following points?
What is the second messenger involved in vagal bradycardia?
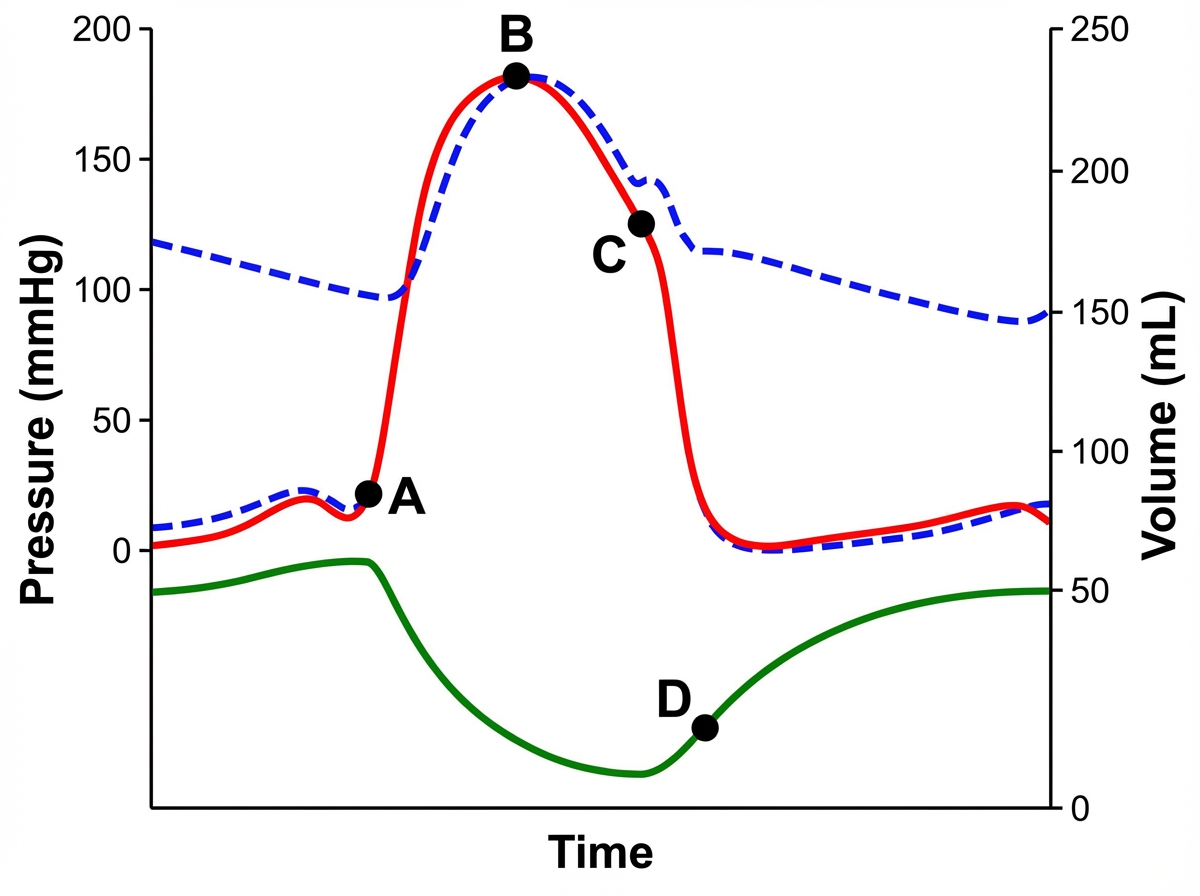
In the cardiac cycle diagram, when does the first heart sound occur?
Which of the following conditions does not cause right axis deviation in ECG?
Edema occurs when plasma protein level falls below which value?
Blood flow to the brain is not influenced by which of the following?
Under normal conditions, the SA node acts as the pacemaker due to which of the following?
A capillary that connects a metaeriole directly with a venule is called as?
Which of the following is a better predictor of vagal tone?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app