
Cardiovascular System — MCQs

On this page
Which of the following phases is absent in the action potential of pacemaker cells?
Which peptide causes increased capillary permeability and edema?
Which of these changes in fetal circulation happen immediately at birth?
A patient's ECG shows Lead III with no S wave, but normal P, R, and T waves. What conclusions can be drawn about the patient's cardiac status?
What period does ventricular contraction correspond to on an ECG?
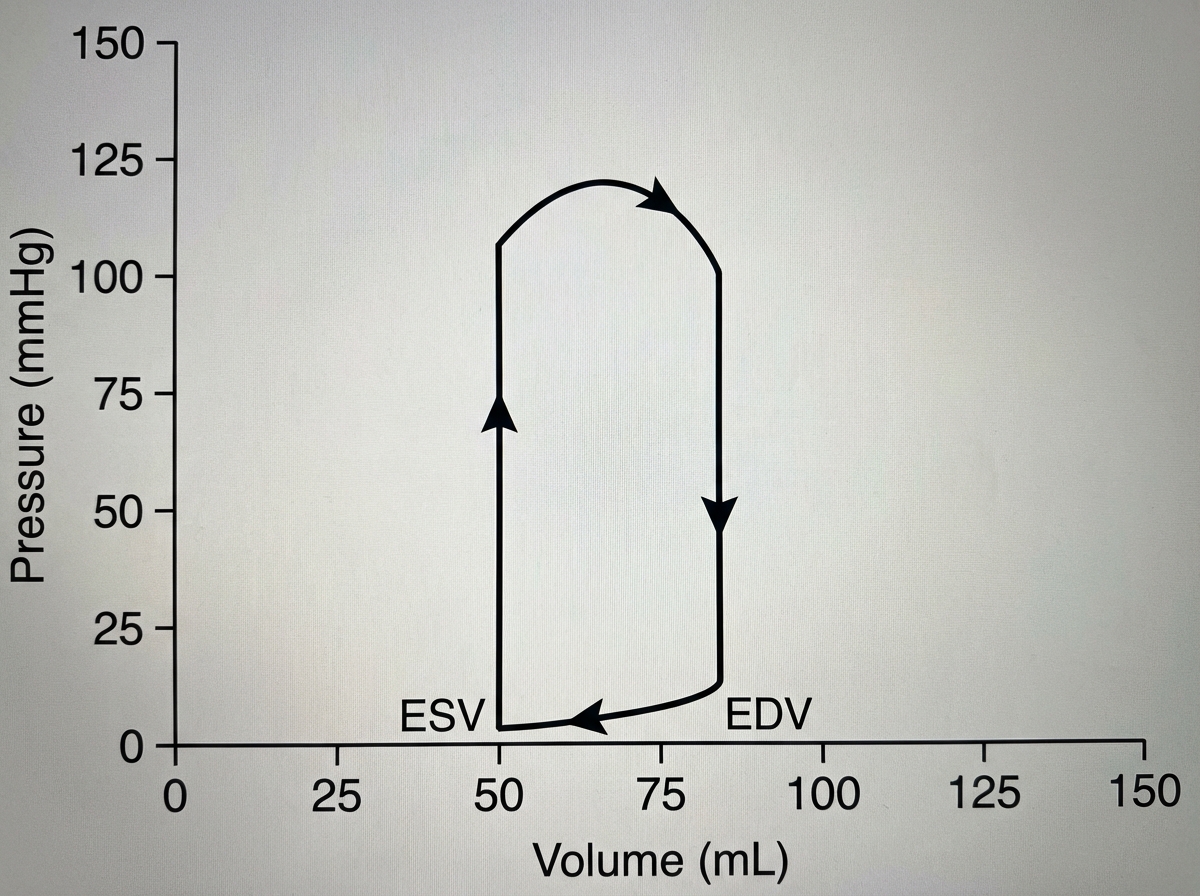
A 40-year-old man presents with a resting heart rate of 180 beats/min. A pressure-volume diagram of the left ventricle is shown below. The end-diastolic volume (EDV) is 85 mL and the end-systolic volume (ESV) is 50 mL. What is the cardiac output?
Which one of the following neurotransmitters functions to increase cardiac output?
During exercise, what happens to blood flow to the brain?
Which of the following causes vasoconstriction in all vascular beds?
Pacemaker potential occurs due to which of the following?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app