
Cardiovascular System — MCQs

On this page
Which formula correctly represents venous return (VR)?
Which component of systemic arterial blood pressure undergoes the least fluctuation?
Which of the following causes a decrease in blood pressure?
What percentage of the total blood volume is typically found in the capillaries?
What is the normal cerebral blood flow per 100 grams of brain tissue per minute?
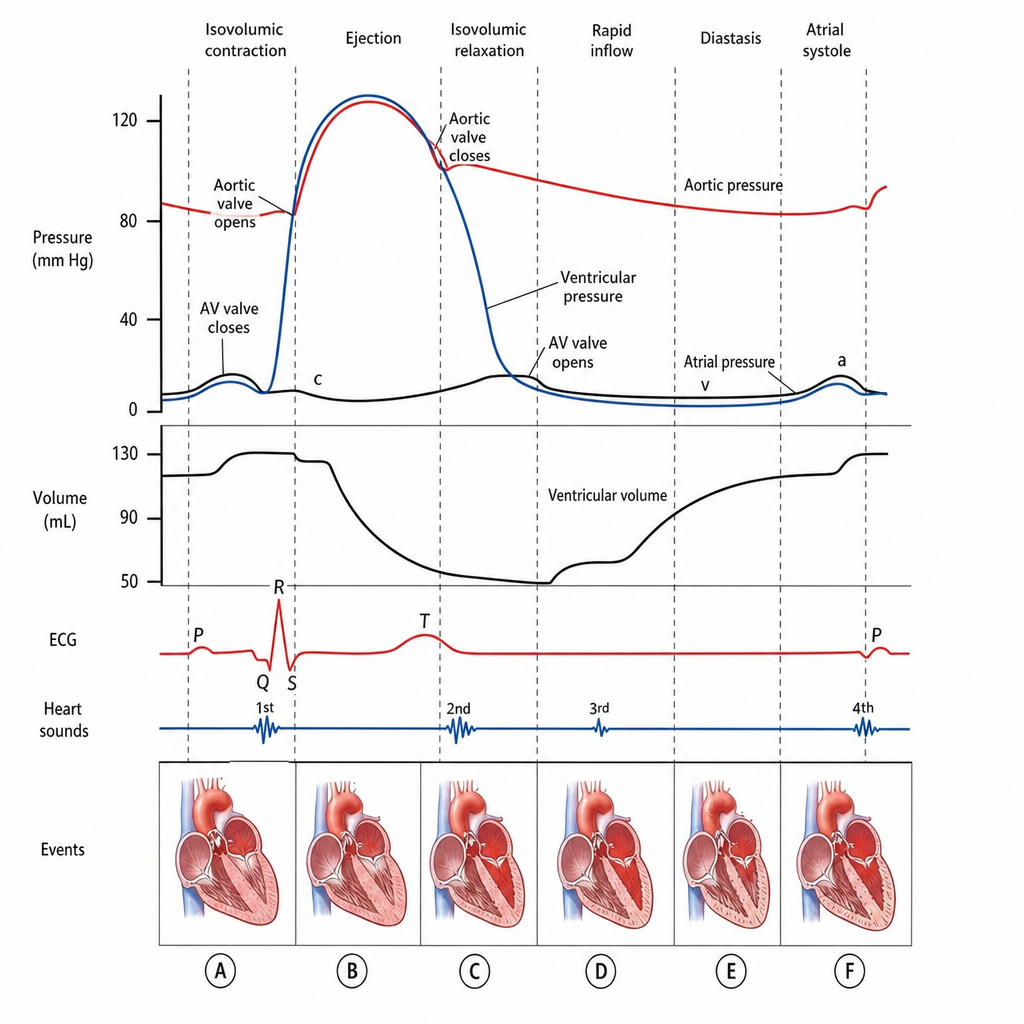
Ventricular filling begins at which point?
Lymph flow from the foot is:
Which of the following is expected to increase in response to hemorrhage?
Which of the following causes an increase in conduction velocity of impulse through the heart?
Calf compartment pressure rises to _________ on walking?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app