
Cardiovascular System — MCQs

On this page
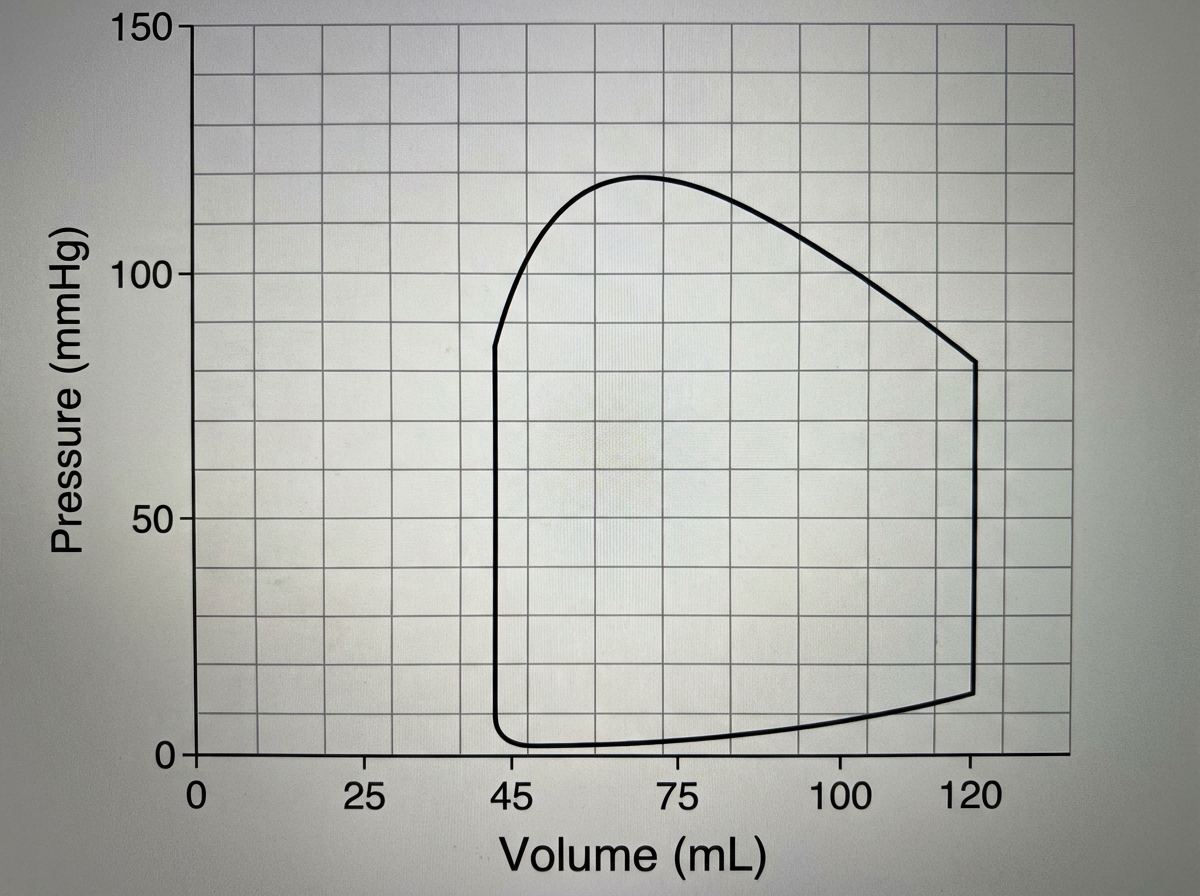
If the heart rate is 70 beats/min, then the cardiac output of this ventricle is closest to?
Which of the following statements regarding blood flow in various organs is true?
If a person has a heart rate of 70 beats/min, a left ventricular end-diastolic volume of 100 ml, and an ejection fraction of 0.50, what is the cardiac output?
Which of the following factors is associated with a decrease in chronic hypertension?
The "incisura" of the arterial pulse corresponds to:
Which wave in the jugular venous pulse represents the atrial relaxation?
The isovolumic relaxation phase of the cardiac cycle ends with which event?
Preload to the heart depends upon which of the following?
Which of the following statements regarding Purkinje fibers is true?
The 'vulnerable period' during cardiac excitation coincides with which of the following?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app