
Cardiovascular System — MCQs

On this page
A patient has an oxygen consumption of 240 ml/min, a pulmonary vein oxygen concentration of 180 ml/L of blood, and a pulmonary artery oxygen concentration of 160 ml/L of blood. What is the cardiac output in L/min?
The 'red reaction' in the triple response is due to which of the following mechanisms?
Baroreceptor stimulation would result in what change?
What is the function of the Wenckebach bundle?
Which of the following is not a measure of stroke volume?
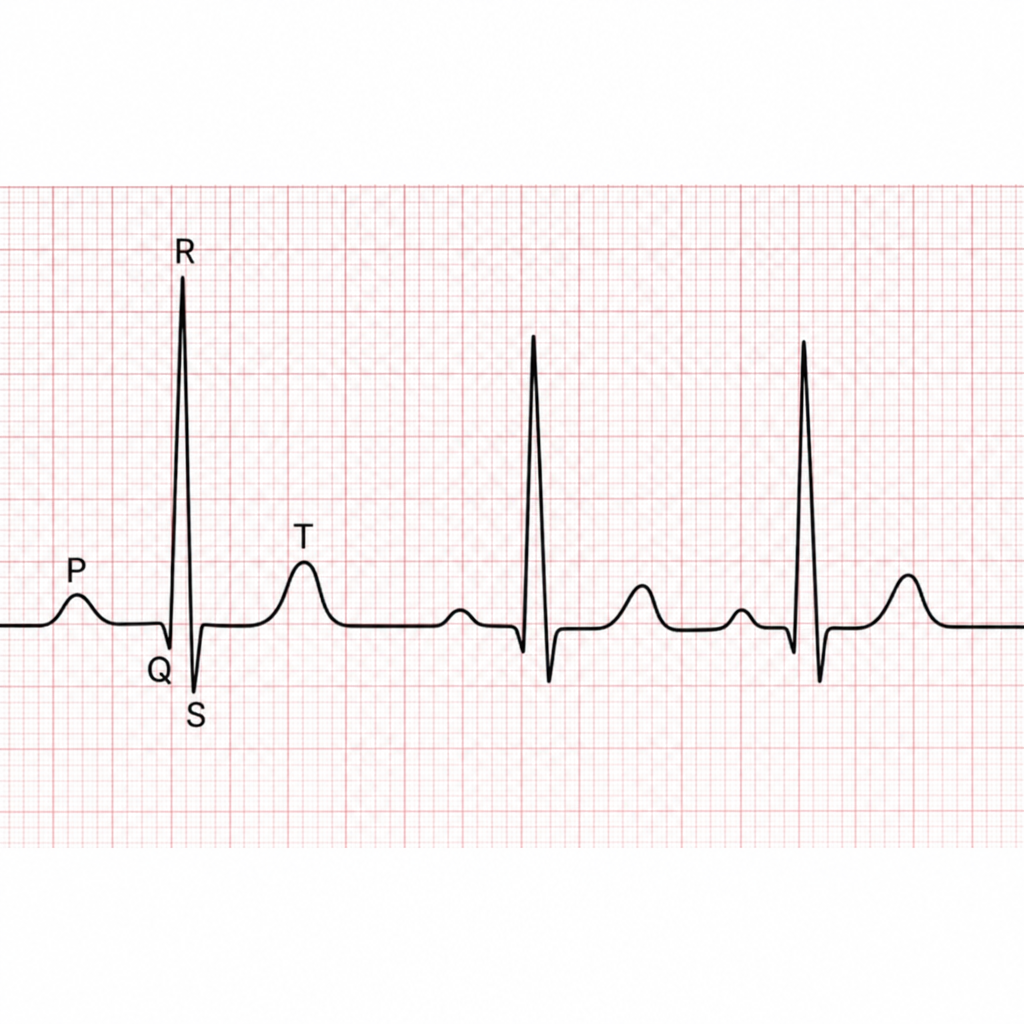
The P wave shown in the ECG represents which of the following?
Isovolumetric relaxation proceeds during which phase of the cardiac cycle?
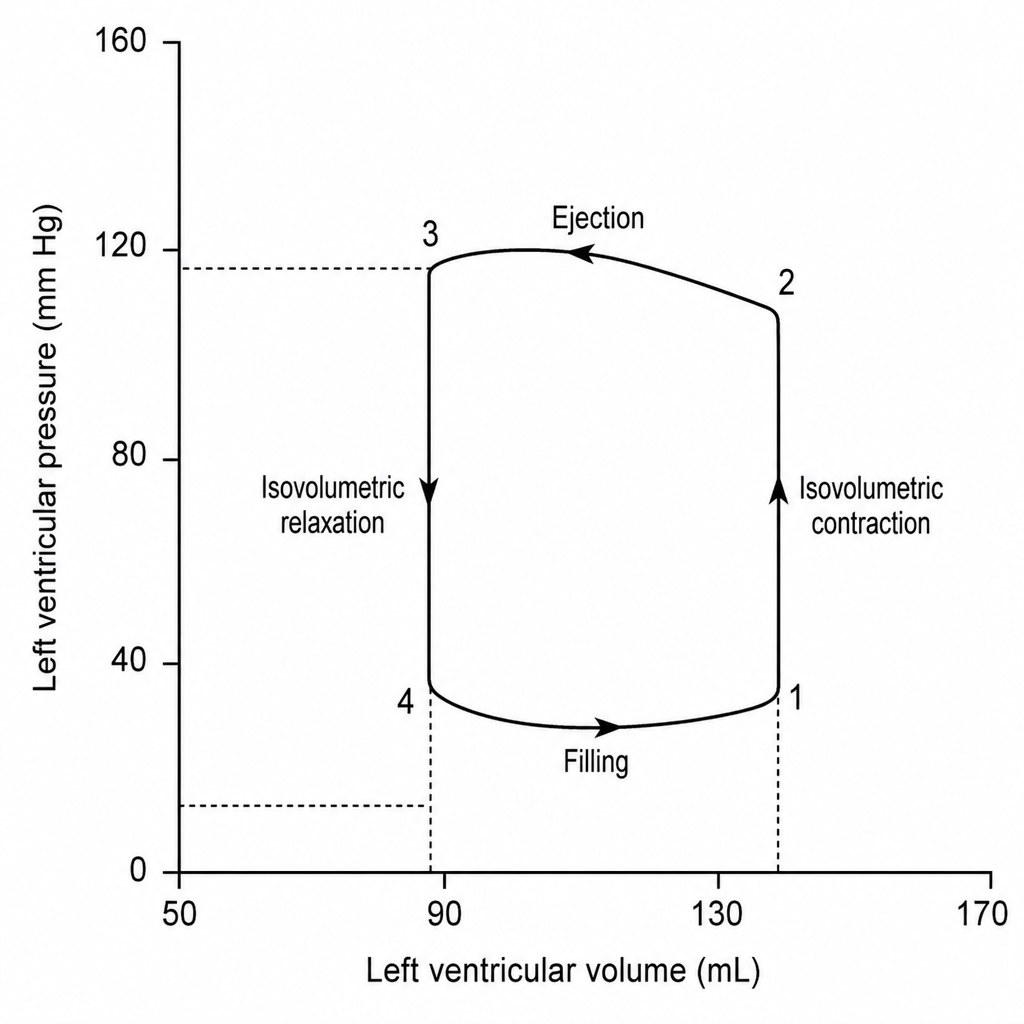
From the left ventricular pressure-volume loop, calculate the ejection fraction.
What does the inward flow of Na+ in the heart lead to?
Which of the following causes maximal cerebral vasodilation?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app