
Cardiovascular System — MCQs

On this page
Stimulation of peripheral chemoreceptors causes which of the following changes in heart rate?
What is the normal pressure in the superficial venous system of the leg while walking?
What is the cause of edema?
A -wave in Jugular Venous Pressure (JVP) indicates which of the following?
A 50-year-old male patient presents with palpitations. Examination of the pulse reveals an irregular heartbeat, and an ECG is advised. The cardiac impulse spreads fastest in which of the following structures?
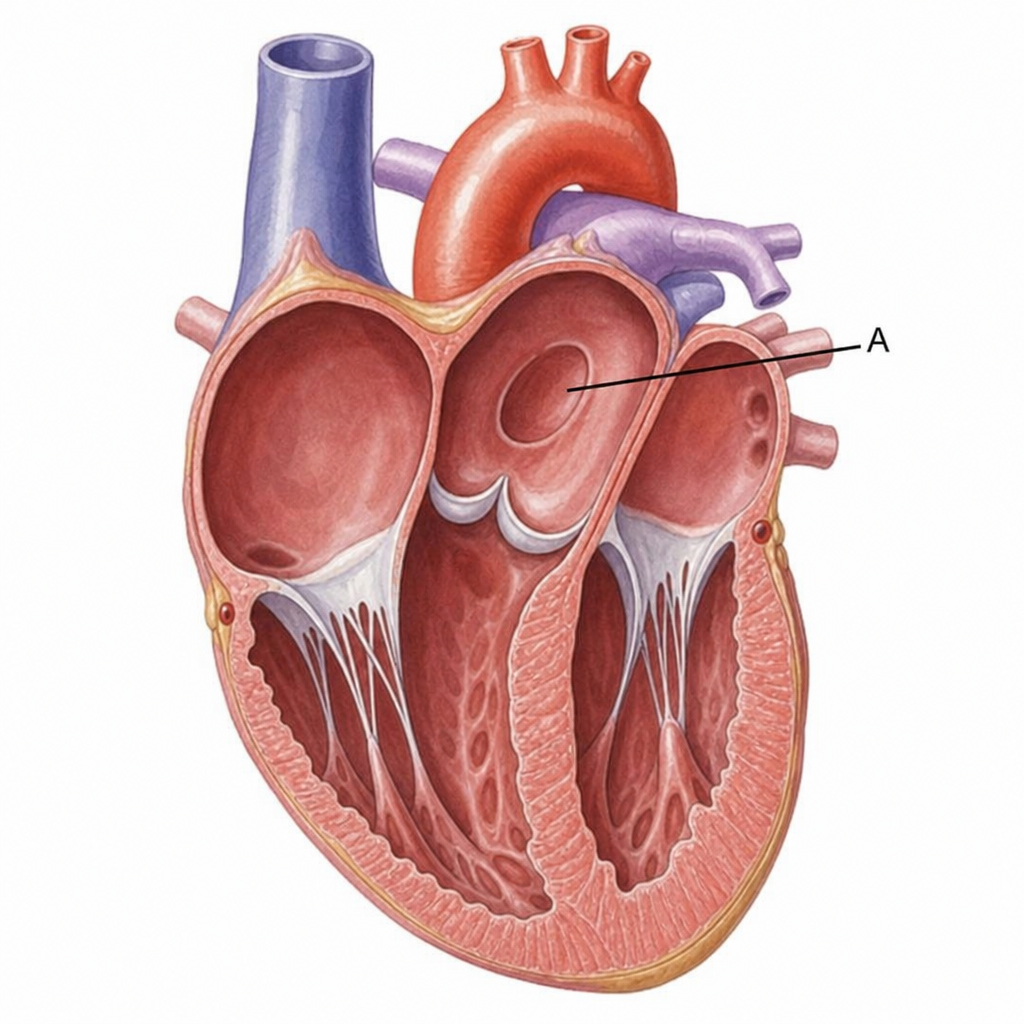
The structure marked A begins to close by what time frame and due to what cause?
Isovolumetric relaxation ends immediately after which of the following events?
What is the most important function of the microcirculation?
Isovolumetric relaxation precedes which of the following events in the cardiac cycle?
What is pulse pressure?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app