
Cardiovascular System — MCQs

On this page
Which of the following is NOT observed in the Bezold-Jarisch reflex?
The normal P wave is inverted in which lead?
What is the resting pacemaker potential in cardiac tissue (in mV)?
All of the following inflammatory mediators produce vasoconstriction except?
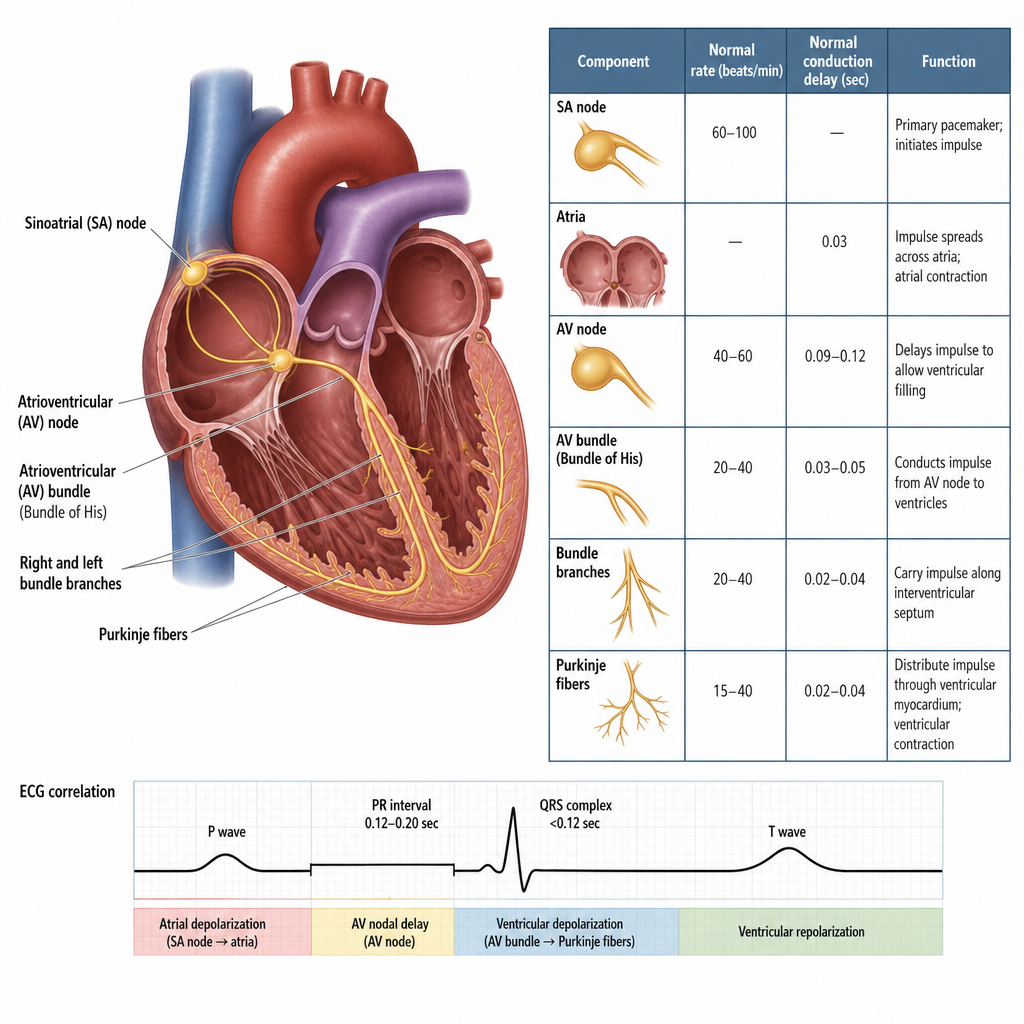
A 55-year-old man has been diagnosed with Stokes-Adams syndrome. Two minutes after the onset of a syncopal attack, which of the following is the pacemaker of the heart?
The chemoreceptor reflex primarily causes which of the following physiological responses?
Which of the following statements regarding cardiac conduction functions are TRUE/FALSE? a) SA Node is the normal primary pacemaker of the heart b) AV Node is not normally the primary pacemaker of the heart c) AV Node is the Gateway to the Ventricles (delays and regulates conduction to the ventricles) d) Purkinje Fibers are located in the Atria e) Bundle of His is the only normal anatomical connection between Atria and Ventricles, traversing the fibrous skeleton
All of the following are true about cardiac muscles, EXCEPT:
A 65-year-old man had an ECG after a biking accident. His QRS voltage was 0.5 millivolt in lead I and 1.5 millivolts in lead III. What is the QRS voltage in lead II?
All are true about nitric oxide except?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app