
Cardiovascular System — MCQs

On this page
Myocardial oxygen demand depends upon which of the following factors?
What effect does parasympathetic stimulation have on the heart?
Ejection fraction increases with:
Regarding the calculation of stroke volume, which of the following statements is NOT true?
The 'C' wave in the Jugular Venous Pulse (JVP) waveform represents which event?
Which of the following is most appropriate regarding the regulation of coronary circulation?
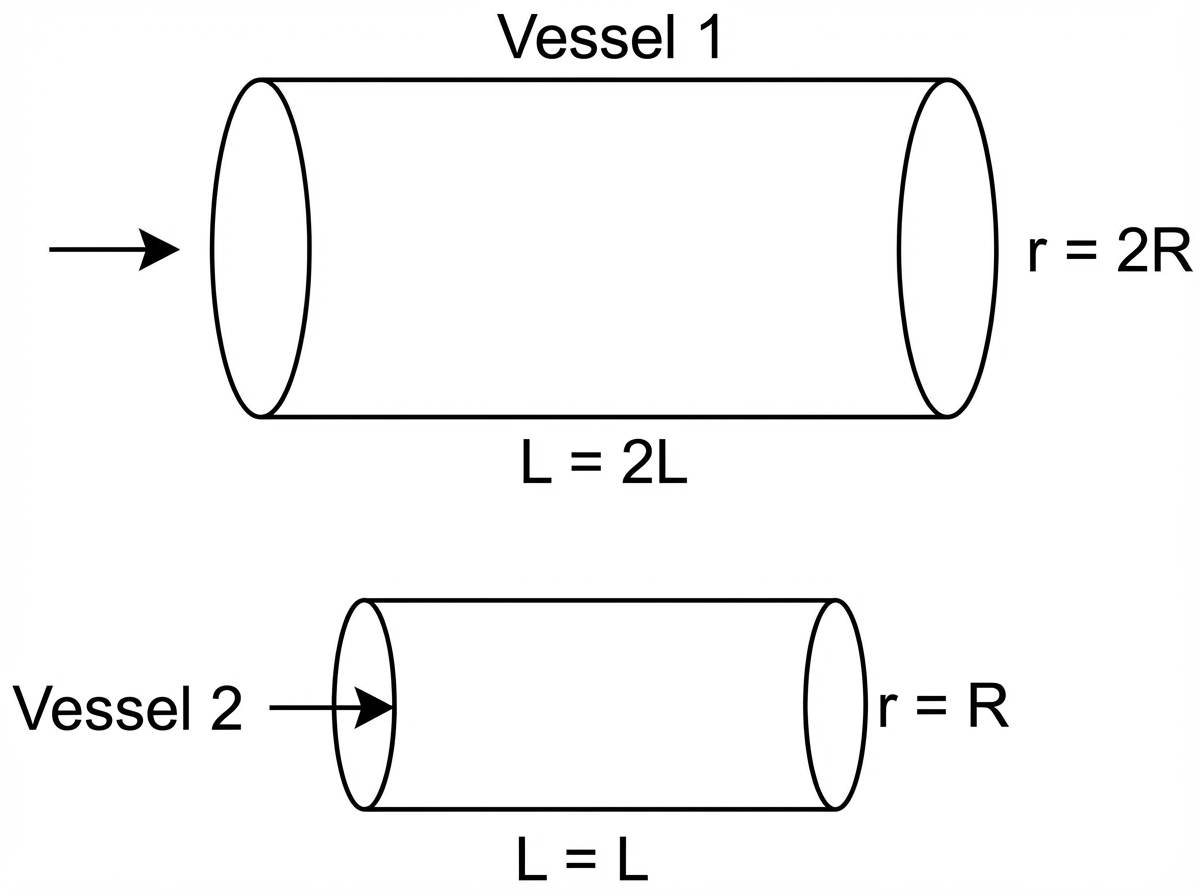
Two vessels are compared as shown in the diagram. Assuming equal pressure drops across both vessels, equal fluid viscosity, and steady laminar flow, what will be the flow across vessel 1 compared to vessel 2?
Mean aerial pressure is calculated as:
Epinephrine increases heart rate by its action on which of the following?
Edema may be caused by any of the following, EXCEPT:
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app