
Cardiovascular System — MCQs

On this page
Edema is due to which of the following factors?
The Bezold-Jarisch reflex causes apnea followed by rapid breathing, hypotension, and bradycardia. Where are the receptors that produce this reflex located?
Compensatory mechanisms during acute hemorrhage include:
What is the state at the end of ventricular diastole?
The ECG of a 40-year-old male was recorded using standard bipolar limb leads. The sum of the voltage of the three standard leads was found to be 5 millivolts. What does this indicate?
Maximum blood flow per 100 gm of tissue is observed in which organ?
Which of the following is responsible for the Bezold-Jarisch reflex?
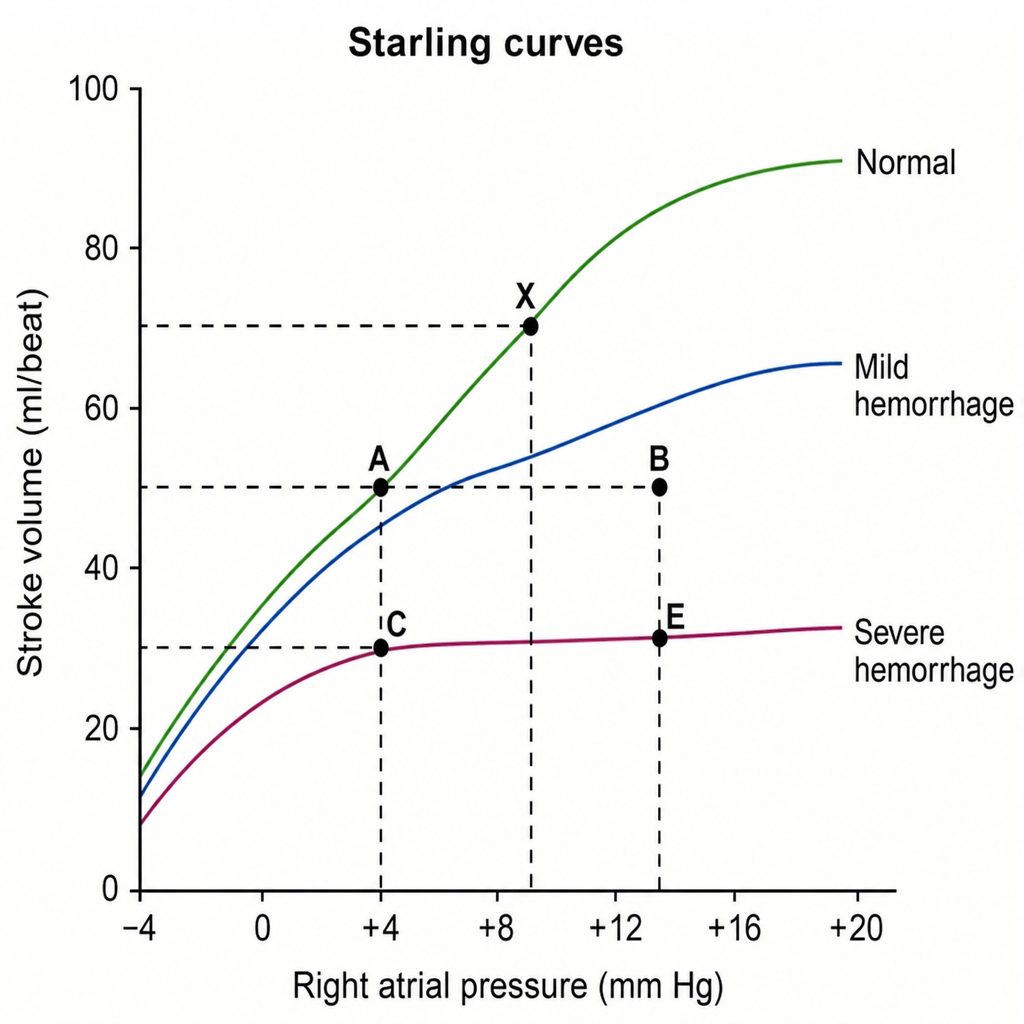
In a graph illustrating Starling's curves, a mild hemorrhage would cause the stroke volume to shift from point X to which point?
In hypovolemic shock, which of the following occurs EXCEPT?
What is true about the third heart sound?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app