
Cardiovascular System — MCQs

On this page
During inhibition of the SA node by vagal stimulation, which of the following occurs?
Cardiac output is measured by all methods EXCEPT?
What is the primary function of lymphatic vessels?
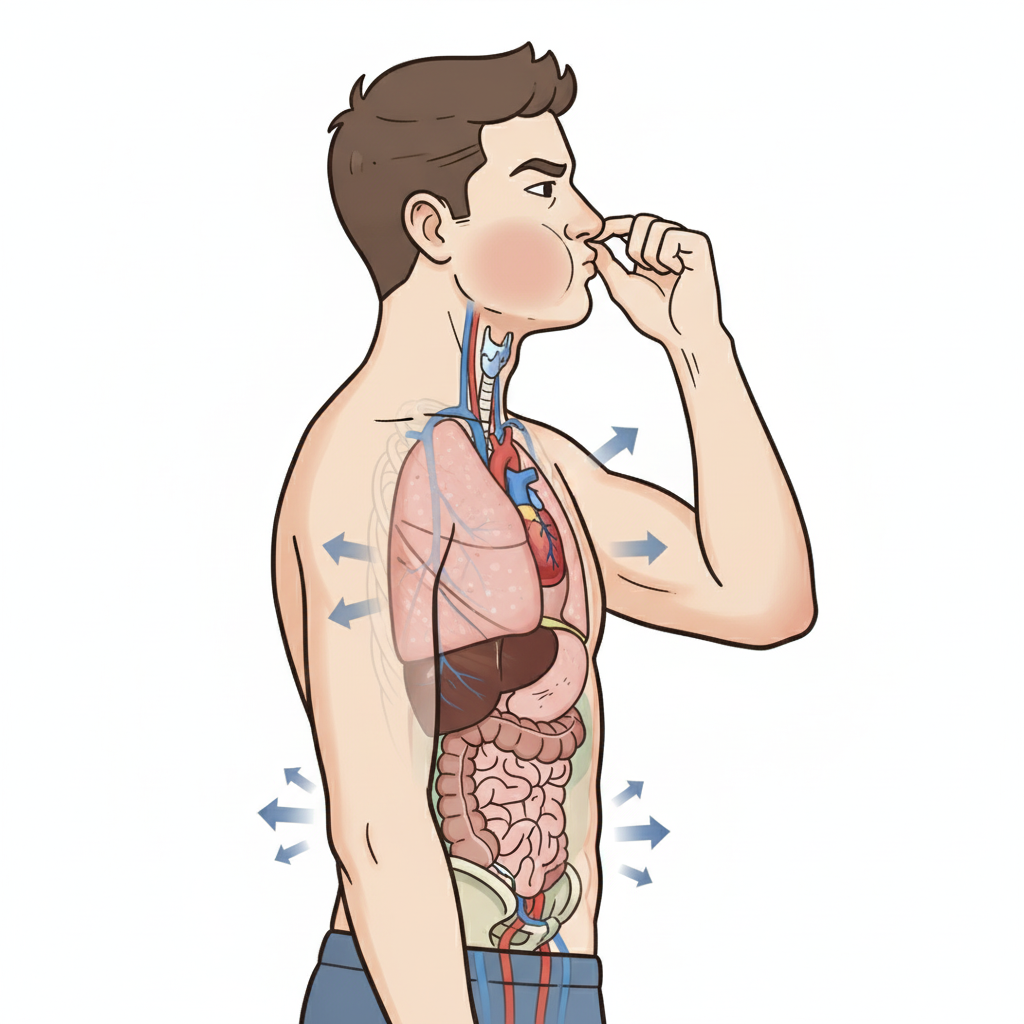
All of the following are physiological effects of early phase II of the manoeuvre shown below except?
What is the normal cardiac index in an adult?
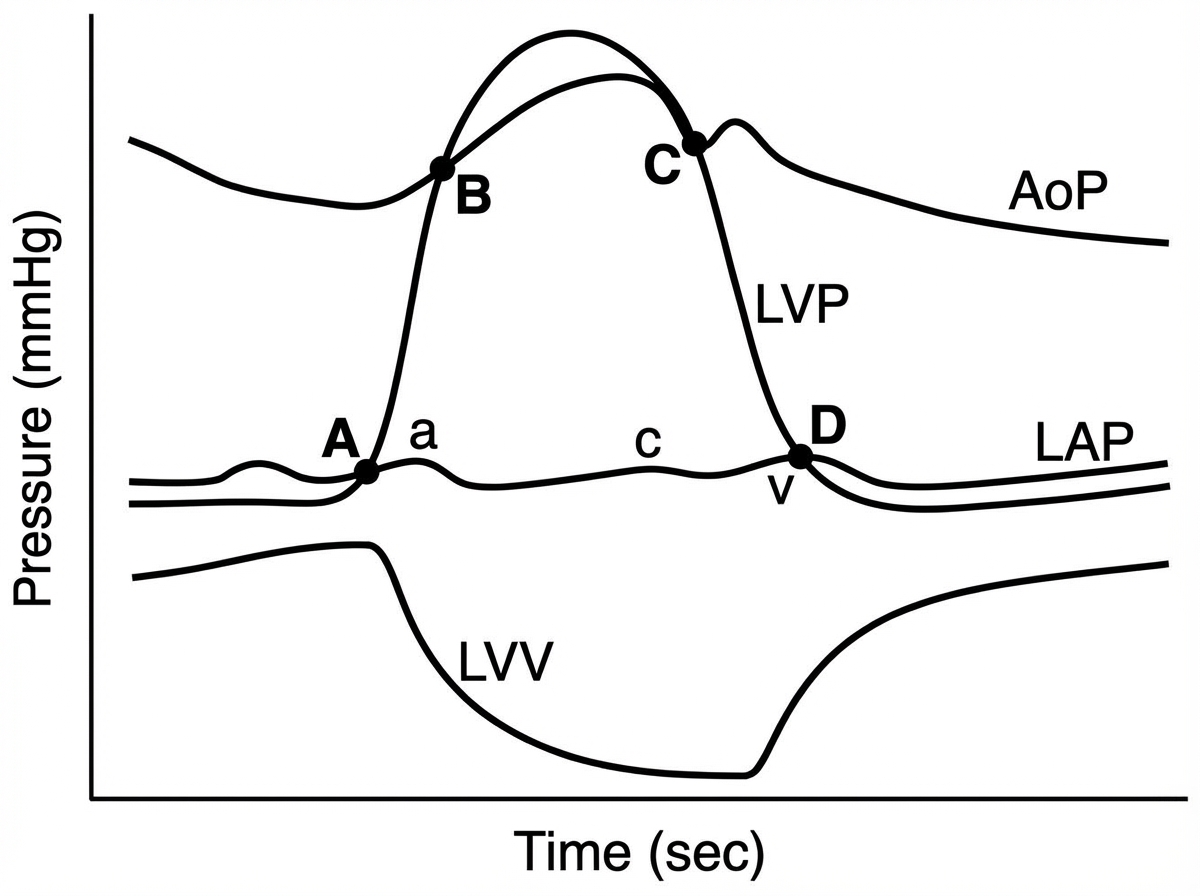
Closing of the mitral valve begins at which point?
Cushing's phenomenon is characterized by which of the following combinations?
Major portion of coronary blood flow occurs during which phase of the cardiac cycle?
Cardiac output changes are minimal during which of the following conditions?
Which of the following describes the low-pressure receptors?
Practice by Chapter
Cardiac Electrophysiology
Practice Questions
Cardiac Cycle
Practice Questions
Cardiac Output and Its Regulation
Practice Questions
Hemodynamics and Blood Flow
Practice Questions
Arterial System Physiology
Practice Questions
Microcirculation and Lymphatics
Practice Questions
Venous Return and Central Venous Pressure
Practice Questions
Cardiovascular Reflexes
Practice Questions
Regional Circulations
Practice Questions
Cardiovascular Responses to Exercise and Stress
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app