
Autonomic Nervous System Drugs — MCQs

On this page
Anti-cholinesterases are ineffective against which of the following?
All of the following may cause cycloplegia except?
Which of the following are adverse effects of tocolytic agonists used in pregnancy?
Ergot derivatives are used in all of the following conditions except:
Which alpha-2 agonist is used in the management of glaucoma?
Timolol can be given in all conditions, except:
Atropine is used in all of the following conditions EXCEPT:
Which drug is used to counter the central anticholinergic effect?
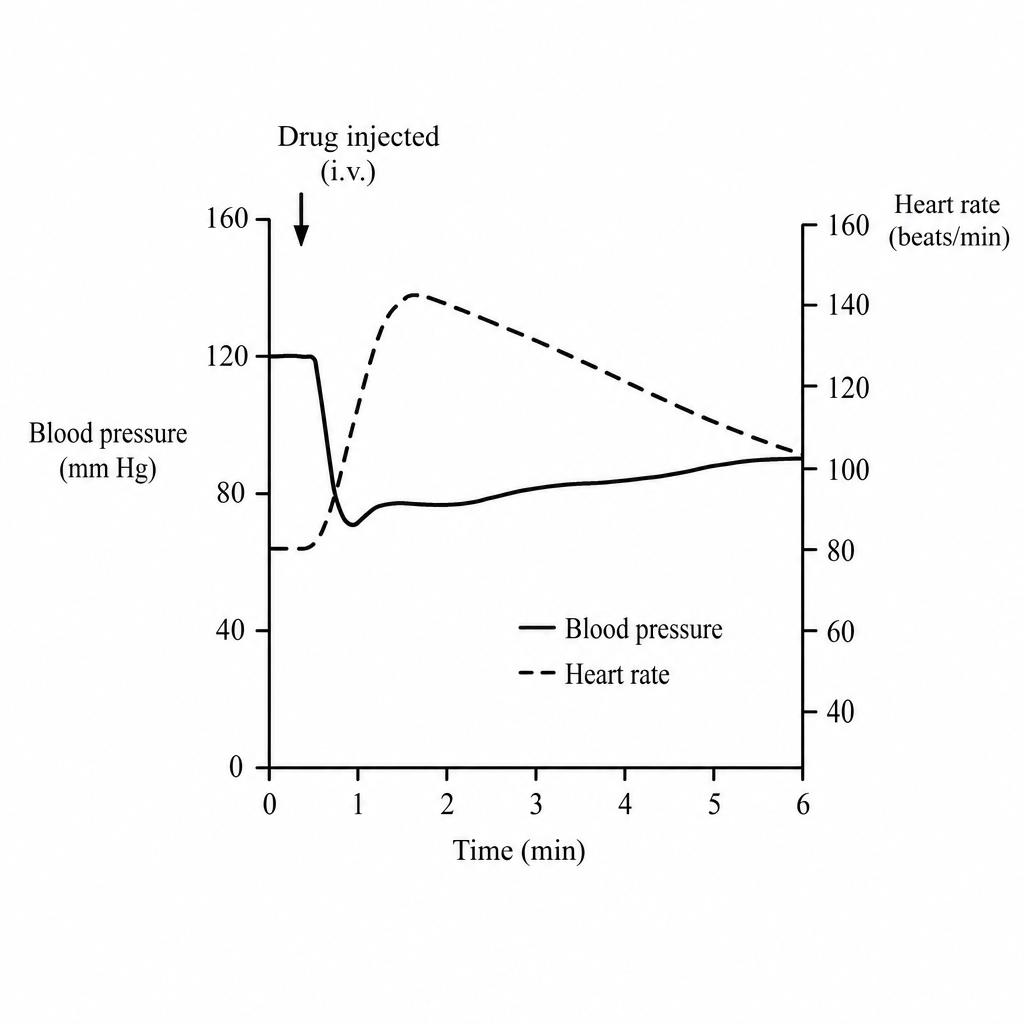
Intravenous bolus dose of a new agonist drug produced the changes in blood pressure and heart rate as shown in the graph. The heart-rate increase persists after autonomic reflex blockade. The most probable receptor affinities of this new drug are?
Which of the following is an anticholinergic used in all EXCEPT?
Practice by Chapter
Cholinergic Agonists
Practice Questions
Cholinergic Antagonists
Practice Questions
Adrenergic Agonists
Practice Questions
Adrenergic Antagonists
Practice Questions
Ganglionic Agents
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Autonomic Drugs in Ophthalmology
Practice Questions
Autonomic Drugs in Cardiovascular Disease
Practice Questions
Autonomic Drugs in Respiratory Disease
Practice Questions
Autonomic Drugs in Urological Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app