
Autonomic Nervous System Drugs — MCQs

On this page
Which of the following statement is correct regarding the mechanism of action of labetalol?
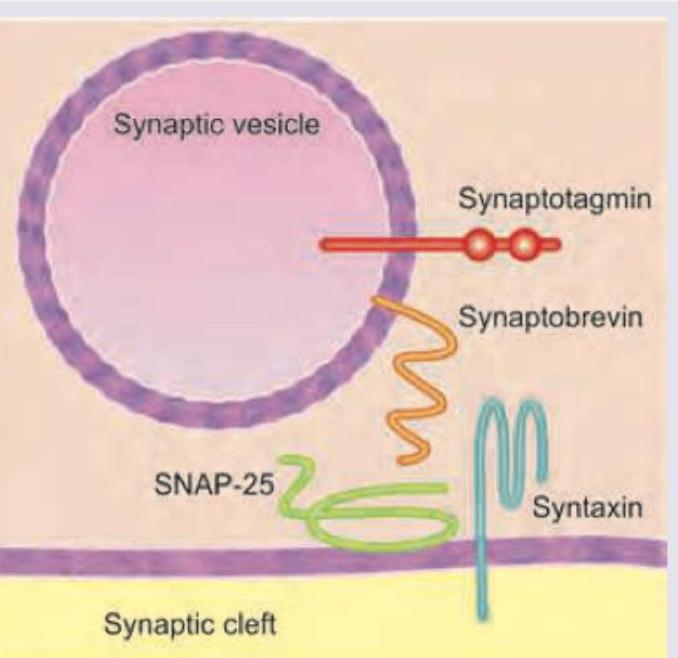
Which of the following is the site of action of botulinum toxin? (Recent NEET Pattern 2016-17)
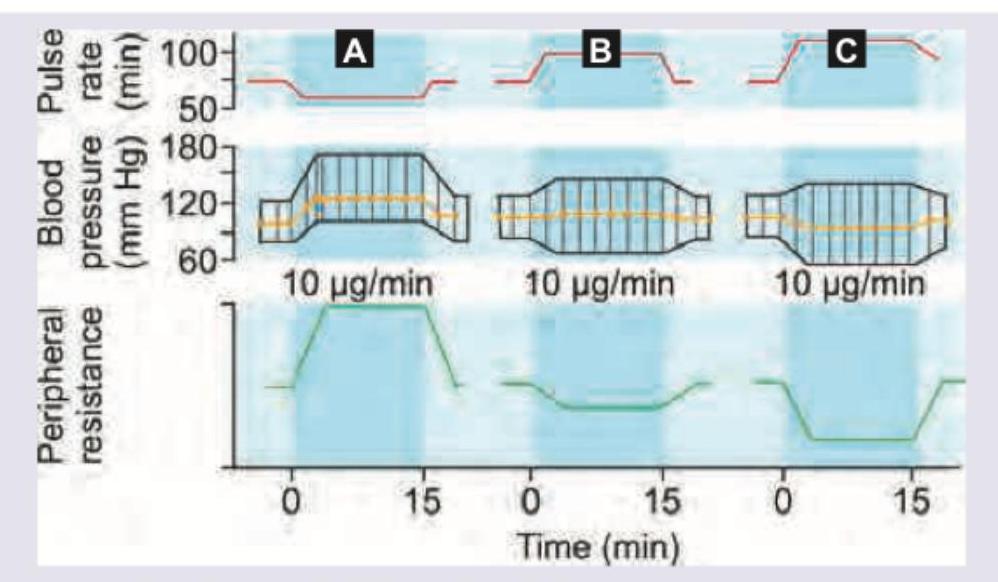
Which of the following statement is correct regarding the graph shown? (AllMS Nov 2016)
A 25-year-old woman going on a luxury holiday cruise has motion sickness. She is prescribed this transdermal scopolamine delivery patch. All are true about its usage except:

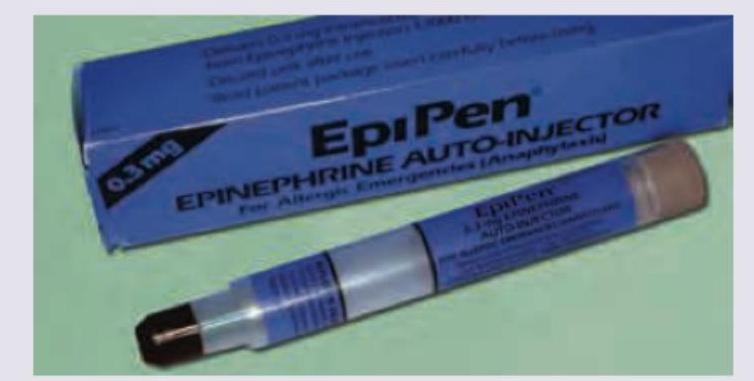
Which of the following conditions can the shown injection be used for emergency management?
Match the following: Column A: a. Beta 1 b. Beta 2 c. Beta 3 Column B: 1. Mirabegron 2. Betaxolol 3. Salbutamol
An investigator is developing a new intravenous medication that acts as a selective agonist at β-2 receptors. In addition to causing bronchodilation, this drug is most likely to have which of the following effects?
Ritodrine is a:-
Shortest-acting muscle relaxant is:
Mechanism of action of atropine in treatment of organophosphate poisoning is?
Practice by Chapter
Cholinergic Agonists
Practice Questions
Cholinergic Antagonists
Practice Questions
Adrenergic Agonists
Practice Questions
Adrenergic Antagonists
Practice Questions
Ganglionic Agents
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Autonomic Drugs in Ophthalmology
Practice Questions
Autonomic Drugs in Cardiovascular Disease
Practice Questions
Autonomic Drugs in Respiratory Disease
Practice Questions
Autonomic Drugs in Urological Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app