
Autonomic Nervous System Drugs — MCQs

On this page
Which anticholinergic agent is commonly used to reverse the action of neuromuscular blockers?
Which skeletal muscle relaxant is preferred in patients with liver and renal disease?
Laudanosine is a metabolite of which neuromuscular blocking agent?
Which one of the following is a contraindication to the use of ergot derivatives?
A diabetic patient with autonomic neuropathy presents with dizziness and hypotension upon waking. What is the drug of choice for this condition?
Which drug is not used in the management of glaucoma?
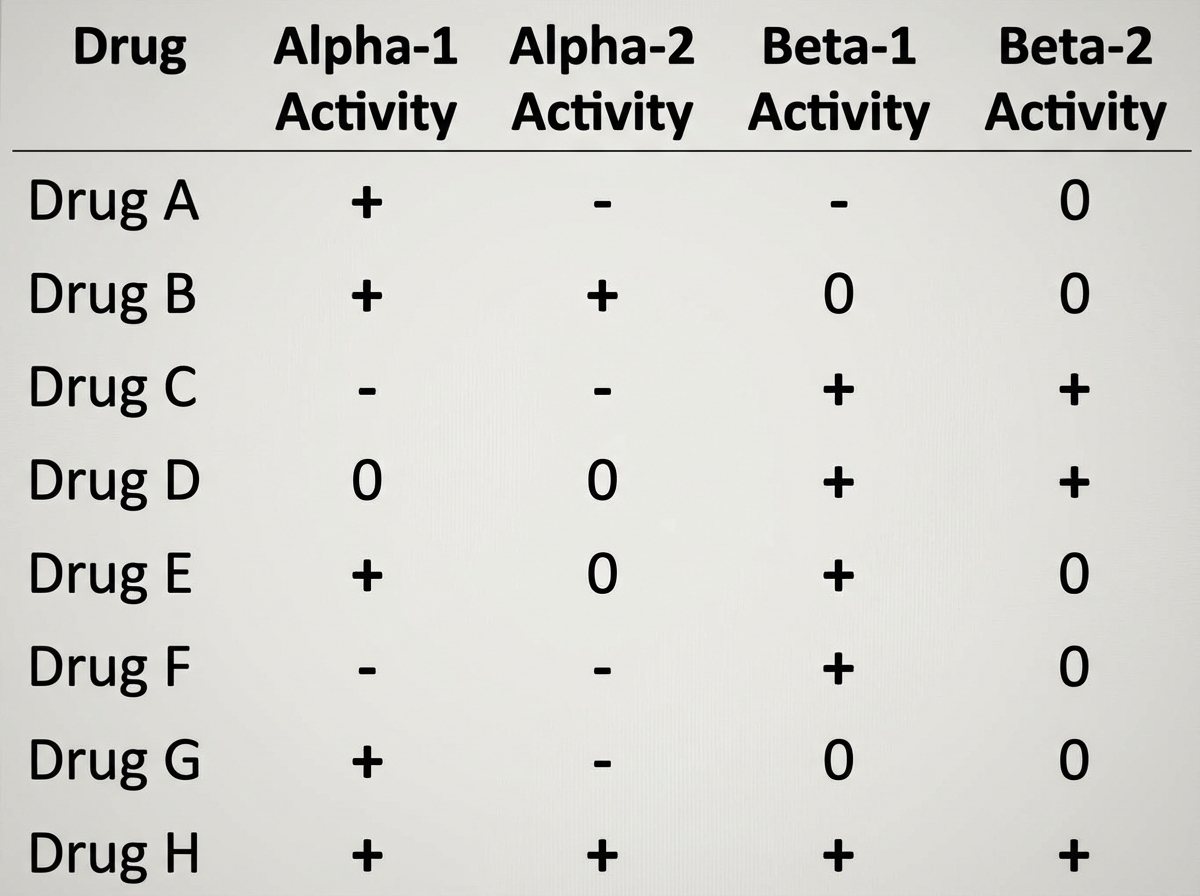
Drug H is most like which of the following agents?
Botulinum toxin affects all of the following except:
Which of the following provides the best explanation for neostigmine being preferred over physostigmine for treating Myasthenia gravis?
Which drug is used to treat dry mouth (xerostomia) in patients undergoing cancer chemotherapy?
Practice by Chapter
Cholinergic Agonists
Practice Questions
Cholinergic Antagonists
Practice Questions
Adrenergic Agonists
Practice Questions
Adrenergic Antagonists
Practice Questions
Ganglionic Agents
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Autonomic Drugs in Ophthalmology
Practice Questions
Autonomic Drugs in Cardiovascular Disease
Practice Questions
Autonomic Drugs in Respiratory Disease
Practice Questions
Autonomic Drugs in Urological Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app